Which of the following statements regarding duodenal atresia are true?
belongs to book: ASIR SURGICAL MCQs BANK|Dr. Gharama Al-Shehri|1st edition| Chapter number:16| Question number:38
All Answers
total answers (1)



belongs to book: ASIR SURGICAL MCQs BANK|Dr. Gharama Al-Shehri|1st edition| Chapter number:16| Question number:38
total answers (1)
 Medicine
Medicine
a. 20% to 40% of these infants have Trisomy 21
c. Bilious vomiting is typical because the obstruction is usually distal to the ampulla of Vater
Twenty to 40% of infants with congenital duodenal obstruction have Trisomy 21. Because this syndrome is not always apparent during the physical examination, a routine karyotype should be obtained. A preoperative ECHO ultrasound examination is also appropriate to evaluate the possibility of associated congenital heart disease. Feeding intolerance and bilious vomiting in the first 24 to 48 hours of life are characteristic. The malformations are typically distal to the ampulla of Vater and thus the infants present with bilious vomiting and proximal duodenal and gastric distention. Malformations proximal to the ampulla of Vater result in nonbilious vomiting and this possibility must not be ignored.
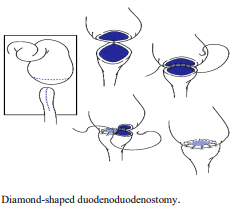
Generally, bypass of the obstructing lesion is the best approach regardless of whether an atresia or annular pancreas is responsible. Division of an annular pancreatic band is inappropriate for two reasons: 1) The duodenum is virtually always atretic in addition. 2) Division of this pancreatic tissue necessarily divides the accessory pancreatic duct within it creating the real possibility of a pancreatic fistula. Generally, the construction of a duodenostomy that minimizes the length of defunctionalized duodenum is preferred. The procedure generally employed is a diamond-shaped duodenostomy. Simple duodenojejunostomy without a Roux-en-Y is occasionally necessary for lesions in the distal duodenum.
need an explanation for this answer? contact us directly to get an explanation for this answer