


BRIEF HISTORY
A 27-year-old man presented to the accident and emergency department with a history of palpitations. He said that he had such palpitations quite often and on two occasions felt dizzy as well. There was no history of fever, chest pain, dyspnoea on exertion, undue intolerance to heat or weight loss. There was no past history of painful swollen joints during adolescent period. He was not a known hypertensive or diabetic. He smoked ten cigarettes a day.
IMPORTANT CLUES ON CLINICAL EXAMINATION
On examination, he looked well and in good health. Pulse was 90 per minute, good volume, regular, and all pulses were palpable. His JVP was not raised and heart sounds were normal. Blood pressure was 125/80 mmHg. His chest was clear. Abdominal and neurological examinations were normal.
INVESTIGATIONS
Investigations were as follows:
| Hb: | 15 g/dl (normocytic normochromic) | Chloride: | 98 mmol/l |
| WBC: |
7.9 × 109 /l P:75% L:20% M:3%E:2% |
Urine: | normal |
| ESR: | 04 mm in 1st hour | Chest X-ray: | normal |
| Platelets: | 290 × 109 /l | ECG | as shown in Figure 4.1 |
| Sodium: | 138 mmol/l | Echocardiogram | normal |
| Potassium: | 4.8 mmol/l | ||
| Bicarbonate: | 24 mmol/l |
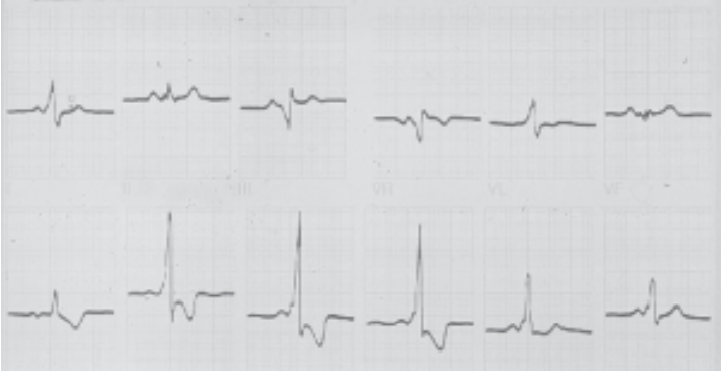
Fig. 4.1: Wolff-Parkinson-White syndrome
QUESTIONS
Q.1. What is the diagnosis in this case?
Q.2. What are the characteristic changes on ECG?
Q.3. Where is the abnormality?
Q.4. What is the treatment?
Q.5. What are the other associations of this condition?
 Medicine
Medicine
ANSWERS
A.1. With history of palpitations in a young man with no other systemic involvement and a clue on ECG favours a diagnosis of Wolff-Parkinson-White syndrome (WPW syndrome).
A.2. The P wave is normal, P-R interval is short (less than 0.12 sec) and there is a little slur (delta wave) on the ascending limb of QRS complex, which may be broad as well. There is a pronounced tendency for the occurrence of atrial tachyarrhythmias which may lead to ventricular tachyarrhythmia, e.g. ventricular tachycardia and ventricular fibrillation.
A.3. There are accessory conduction pathways from atria to ventricles bypassing the AV node. They are three in number namely—bundle of Kent, bundle of James and bundle of Mahaim. Short circuiting occurs and the patient gets tachyarrhythmias including supra-ventricular and ventricular tachycardia which can progress to ventricular fibrillation and death.
A.4. This may be medical and consists of those drugs which prolong refractory period of cardiac conduction tissue, e.g. amiodarone (Cordarone). For surgical treatment, electrophysiological study of the heart is important and tractectomy by cryorsurgery is done. Radioablation may also be an option.
A.5. Pre-excitation syndrome is associated with Ebsteins and other cardiac anomalies, e.g. mitral valve prolapse, hypertrophic cardiomyopathy.
NB: WPW syndrome should be differentiated from LGL syndrome (Lown-Ganong-Levine syndrome) in which there is normal p-wave, short PR interval, short QS interval, but there is no delta-wave on the ascending limb of QRS complex.
need an explanation for this answer? contact us directly to get an explanation for this answer