


0
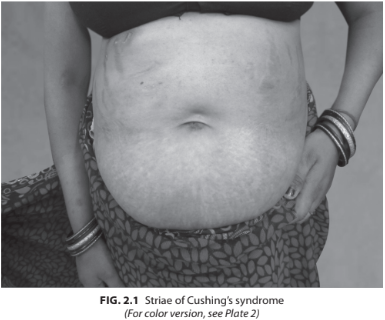
A 29-year-old female presented with progressive swelling over the body, weight gain, menstrual irregularity. On examination, her BP was 160/100 mm Hg, pulse rate 86/min, weight 88 kg, height 155 cm. Buffalo hump was present with broad purplish striae over the abdomen. Proximal muscle weakness was present. Her investigations revealed Hb 12.6 g%, fasting blood sugar (FBS) 170 mg%, creatinine 0.9, Na 140 mEq/L, K 3.4 mEq/L (Fig. 2.1).
What are the treatment modalities for Cushing’s syndrome?
 Medicine
Medicine
• Treatment is based on the source of the hypercortisolism, so the need for an accurate diagnosis cannot be overemphasized. The goal of treatment is to reverse the clinical manifestations of hypercortisolemia by decreasing cortisol secretion to normal levels.
• In exogenous Cushing’s syndrome, gradual withdrawal of the glucocorticoid is important because most patients on long-term therapy will have some degree of HPA-axis suppression with resultant adrenal insufficiency if therapy is abruptly discontinued.
• In ACTH-independent Cushing’s syndrome, adrenal imaging by either CT or MRI will demonstrate unilateral or bilateral disease. Patients should be referred for adrenalectomy. During and after unilateral adrenalectomy, patients should receive glucocorticoid replacement until the HPA axis recovers from the prolonged suppressive effects of glucocorticoid excess. Patients with bilateral adrenalectomy require lifelong glucocorticoid and mineralocorticoid replacement.
• In Cushing’s disease, a trans-sphenoidal pituitary surgery is the treatment of choice for patients with a clearly circumscribed microadenoma. In other cases, subtotal resection of the anterior pituitary may be performed. Patients with incomplete resection of the tumor may undergo repeat surgery or pituitary irradiation with either conventional radiation or stereotactic radiation with the gamma knife. Pituitary irradiation may not control the hypercortisolemia for months to years, and patients require medical therapy until the full effects of the radiation take effect. Surgical cure with transsphenoidal adenomec-tomy can be assessed on postoperative day 2–3 with morning cortisol levels, which are undetectable with successful complete resection of the tumor. After transsphenoidal resection of the adenoma, patients require glucocorticoid replacement until recovery of the HPA axis (Table 2.3).
• Ectopic ACTH–dependent Cushing’s syndrome should be confirmed with imaging studies, including CT, MRI, and/or scintigraphy. Tumors that can be localized by imaging studies should be removed surgically. If the source is an occult tumor or if there is metastatic disease, medical treatment is required. Bilateral adrenalectomy may be performed in refractory cases.
Surgery
• Preferred treatment modality
• Trans-sphenoidal pituitary resection.
Medical Management
Following are the indications for medical management in Cushing’s syndrome:
• Preoperatively to control cortisol levels
• Patients in whom surgery is contraindicated
• Patients in whom surgery/radiotherapy has failed
• Awaiting effect of radiotherapy to take place
• Ketoconazole is an antifungal agent that inhibits 17, 20-lyase, 11-β-hydroxylase, and cholesterol side-chain cleavage enzyme. It is usually the first-line medication. Its cortisol-reducing effects are dose-dependent and can be seen rapidly. The major side effect is liver toxicity. Other side effects include gynecomastia, impotence, and gastrointestinal symptoms. Doses range from 200 to 1200 mg orally daily in 2–3 divided doses.
• Mitotane inhibits cholesterol side-chain cleavage enzyme and 11-β-hydroxylase. Mitotane induces permanent destruction of adrenocortical cells and, therefore, can be used to achieve medical adrenalectomy as an alternative to surgical adrenalectomy. Glucocorticoid replacement is started at initiation of mitotane treatment. Mineralocorticoid treatment may eventually be required. Side effects are generally dose dependent and include gastrointestinal symptoms, weakness, lethargy, leukopenia, gynecomastia, and hypercholesterolemia. Doses start at 0.5 g orally at bedtime and are increased slowly to 2–3 g/day in 3 to 4 divided doses for a total of 6–9 months.
• Metyrapone inhibits 11-β-hydroxylase. Major side effects include increased androgens, hypertension, and hypokalemia through increased 11-deoxycorticosterone. Doses range from 250 to 1000 mg orally, given every 6 hours. Lower doses of 500–750 mg orally daily can be used when given in combination with ketoconazole and/or aminoglutethimide.
• Aminoglutethimide is an anticonvulsant that inhibits the cholesterol side- chain cleavage enzyme. The usual dose is 250 mg 2–3 times a day. Side effects include gastrointestinal upset, lethargy, ataxia, hypothyroidism, headache, bone marrow suppression, and skin rash. It is not as effective for monotherapy as ketoconazole or metyrapone, and thus is frequently used in combination with other agents.
• Other agents with limited or modest anticorticosteroid capabilities include Mifepristone (RU486), somatostatin receptor ligands (octreotide, lanreotide, pasireotide), Etomidate, and dopamine receptor agonists (bromocriptine or cabergoline).
Radiotherapy
Indication: Residual disease after initial pituitary surgery. Fractionated external beam radiotherapy or stereotactic radiosurgery achieves control of hypercortisolism in approximately 50–60% of patients within 3–5 year. Long-term follow-up is necessary to detect relapse, which can occur after an initial response to both types of radiotherapy. The incidence of therapy-induced pituitary failure appears to be similar with radiotherapy or radio- surgery. Insufficient studies are available to evaluate the effects of radiotherapy on cerebrovascular and neurocognitive functions. The risk of second tumor formation after pituitary radiation is considered to be in the range of 1–2%.
need an explanation for this answer? contact us directly to get an explanation for this answer