


0
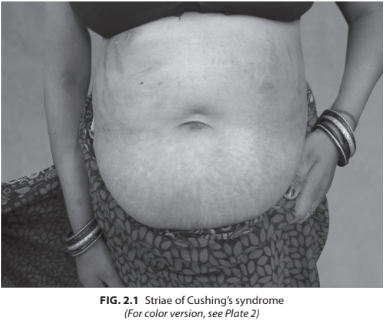
A 29-year-old female presented with progressive swelling over the body, weight gain, menstrual irregularity. On examination, her BP was 160/100 mm Hg, pulse rate 86/min, weight 88 kg, height 155 cm. Buffalo hump was present with broad purplish striae over the abdomen. Proximal muscle weakness was present. Her investigations revealed Hb 12.6 g%, fasting blood sugar (FBS) 170 mg%, creatinine 0.9, Na 140 mEq/L, K 3.4 mEq/L (Fig. 2.1).
What could be other problems/complications associated with Cushing’s disease?
 Medicine
Medicine
Progressive central obesity involving the abdomen, face, and neck (buffalo hump, moon facies, supraclavicular fat pads, and exophthalmos from retro- orbital fat deposition).
Metabolic complications include glucose intolerance (owing to stimulation of gluconeogenesis by cortisol and peripheral insulin resistance caused by obesity), and hypertension (through poorly understood multifactorial etiologies), both of which confer increased cardiovascular risk, a major cause of morbidity and death in patients with Cushing’s syndrome. Severe hypertension and hypokalemia are more commonly seen in patients with ectopic ACTH syndrome because the very high serum cortisol levels overwhelm the capacity of the 11-β-hydroxysteroid dehydrogenase type 2 enzyme, which oxidizes cortisol to inactive cortisone in renal tubules, thereby resulting in activation of mineralocorticoid receptors, hence causing hypokalemic alkalosis. Hypokalemia aggravates hyperglycemia by inhibiting insulin secretion.
Dermatologic manifestations include skin atrophy (thinning of the stratum corneum), hair thinning, fragile skin with easy bruisability, wide purple striae (due to the stretching of fragile skin), cutaneous fungal infections, and hyperpigmentation (in ectopic ACTH syndrome). Reproductive changes include menstrual irregularities, hirsutism, oily facial skin with acne, and other signs of virilization (temporal balding, deepening voice), especially in women with adrenal carcinoma.
Musculoskeletal manifestations are proximal myopathy, muscle wasting (resulting from the catabolic effects of excess glucocorticoid on skeletal muscle as well as aggravated due to resulting hypokalemia), and osteoporosis (caused by decreased bone formation, increased bone resorption, and decreased intestinal and renal calcium reabsorption). Vertebral compression fractures, pathologic fractures of the rib or long bones, and aseptic necrosis of the femoral heads may also be present. Neuropsychiatric changes can include labile mood, agitated depression, anxiety, panic attacks, mild paranoia, impaired short-term memory and cognition, and insomnia.
• Clinical features which are more common in exogenous Cushing’s syndrome are glaucoma, cataract, benign intracranial hypertension, pancreatitis and avascular necrosis of the head of the femur.
• Cushing’s syndrome is more likely, if onset of above feature is at a young age.
It is to be noted spontaneous Cushing’s syndrome is rare, and hence the positive predictive value of any one feature alone is low. In malignant ACTH secreting tumor, there may be cachexia with rapid presentation in comparison to a benign tumor.
In Cushing’s disease, there is usually micropituitary adenoma <10 mm in diameter, and hence visual loss is not present.
need an explanation for this answer? contact us directly to get an explanation for this answer