


0
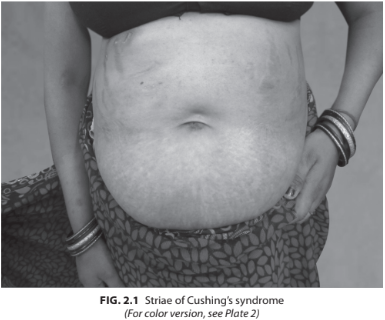
A 29-year-old female presented with progressive swelling over the body, weight gain, menstrual irregularity. On examination, her BP was 160/100 mm Hg, pulse rate 86/min, weight 88 kg, height 155 cm. Buffalo hump was present with broad purplish striae over the abdomen. Proximal muscle weakness was present. Her investigations revealed Hb 12.6 g%, fasting blood sugar (FBS) 170 mg%, creatinine 0.9, Na 140 mEq/L, K 3.4 mEq/L (Fig. 2.1).
How do you further investigate a patient of Cushing’s syndrome?
 Medicine
Medicine
The next line involves two critical steps:
1. Determining, if the cortisol excess is ACTH independent or ACTH dependent (Does the patient have primary adrenal disease or an ACTH-secreting tumor?)
2. If ACTH secreting, then determining the source of the ACTH in the ACTH- dependent form (Does the patient have Cushing’s disease (pituitary adenoma) or ectopic ACTH syndrome?)
Measurement of ACTH
Adrenocorticotropic hormone (ACTH) measurement will help us to differentiate ACTH from the non-ACTH-dependent Cushing’s syndrome. Sample is collected with adequate precautions in the morning at 9:00 AM and measured. Some centers advocate checking the ACTH in the midnight along with the cortisol to interpret and differentiate the two. Morning ACTH value of less than 10 pg/mL is suggestive of an ACTH-independent Cushing’s syndrome. And the value of more than 22 pg/mL is suggestive of ACTH-dependent Cushing’s syndrome. Further testing is required, if the values are equivocal. Patients with equivocal ACTH values between 10 and 20 pg/mL may be subjected to corticotropin-releasing hormone (CRH) stimulation test and the increment of the ACTH and cortisol response are suggestive of Cushing’s disease. High-dose dexamethasone suppression test (HDDST) though used to differentiate the pituitary from ectopic ACTH-dependent Cushing’s syndrome is not definitive. The sensitivity and the specificity depend on the amount of cortisol suppression, and can be suppressed in carcinoid syndrome producing ACTH. Other tests that are available to differentiate the cause of Cushing’s syndrome are given in Table 2.2.
• Adrenocorticotropic hormone values between 10 and 20 pg/mL are subjected to the CRH stimulation to differentiate, but the clinical clues such as pigmentation and imaging have to be considered before coming to a conclusion. Although many tests are available, none of them clearly differentiate the patients with equivocal results. Therefore, a lot of clinical discretion is required and the treating endocrinologist should also be aware of all the pitfalls of the diagnostic tests.
• Adrenocorticotropic hormone molecule is rapidly degraded by the plasma proteases. Hence, it should be collected in a prechilled tube to avoid false low values. So while interpreting the value, ensure proper collection of the sample.
• High-dose dexamethasone suppression test shows suppression by only less than 50% of the basal cortisol value in about 80% of the patients with Cushing’s disease. And there are high numbers of false positive tests (10–30%) in ectopic Cushing’s syndrome.
need an explanation for this answer? contact us directly to get an explanation for this answer