


0
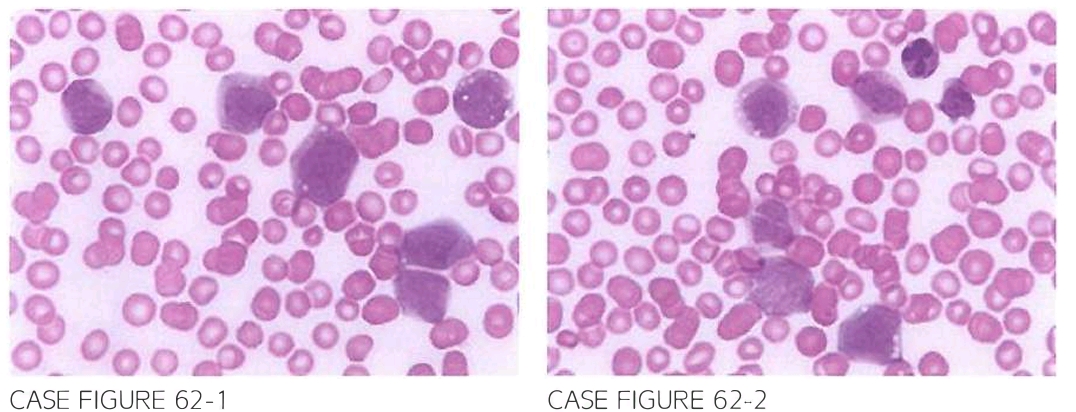
A 32-year-old male presents for evaluation of skin lesions. increased bruising. and fa tigue. Examination reveals a conglomerate of nodular skin lesions involving the skin of the face and upper trunk. There is no hepatosplenomegaly or lymphadenopathy. Dif fuse petechial rash is seen over both lower extremities. Laboratory evaluation reveals leukocyte count of 57.200/ ,LLL. hemoglobin of 7.8 g/dl. and platelet count of 8.000/ ,LLL. Flow cytometry reveals expression of CD11 c. CD13. CD1 LJ, CD33, CD3LJ. CD68. and HLA-DR. Staining for myeloperoxidase (MPO) and nonspecific esterase (NSE) shows positivity in LJO% and LJS%. respectively. Peripheral blood smear is shown below.
What is the most likely diagnosis?
- Acute myeloid leukemia with maturation
- Acute myelomonocytic leukemia (AMML)
- Acute megakaryoblastic leukemia (AMKL)
- Acute myeloid leukemia with minimal differentiation
- Acute promyelocytic leukemia (APL)
 Medicine
Medicine
B. Peripheral slide reveals the presence of myeloid blast cells exhibiting dispersed chroma tin and high nuclear-to-cytoplasmic ratio. The blasts appear to bear morphologic resemblance to monocytes and express monocytic cell surface markers: CD 11 c, CD 14, and CD68. Positive staining for MPO and NSE, in addition to the characteristic skin involvement, is most consistent with AMML. Cutaneous involvement can be seen in 15% of AML cases and is most characteristic of AML with monocytic or myelomonocytic differentiation, where it has been reported in up to 50% of cases. Posi tivity for MPO excludes AML with minimal differentiation because, by definition, these cases are negative for MPO. Monocytic markers are usually absent in cases of AML with maturation. Flow cytometryin cases ofAPLischaracteristicallynegativeforCD34 andHLA-DR (Blood. 20 11; 118( 14):3785, Ann Hematol. 2002;81(2):90, Blood. 1980;55(1):71, Blood. 2011;118(14):3785).
need an explanation for this answer? contact us directly to get an explanation for this answer