


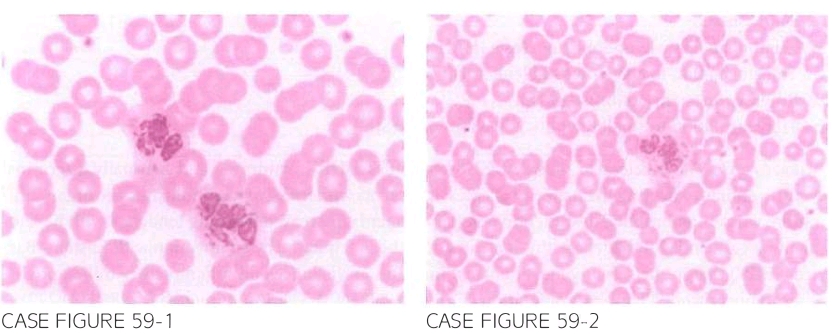
A 8-year-old boy with history of recurrent cutaneous Staphylococcal infections from infancy is referred for further evaluation secondary to an abnormal reported peripheral blood smear review during a recent hospital admission. There is no preceding history of bleeding. Physical examination reveals silver colored hair and mild splenomegaly with no lymphadenopathy. Laboratory workup shows leukocyte count of 6. 700/ J.LL. hemoglobin 12.3 g/dl. and platelet count 376.000/J.LL. Peripheral blood smear is shown below.
Patient is treated conservatively and followed up for the next 2 years till he presents to the emergency department complaining of persistent fever. left-sided abdominal pain, and increased bruising. Patient also reports increased frequency of infections over the preceding 2 months. Physical examination reveals diffuse lymphadenopathy with wors ening splenomegaly and new-onset moderate pancytopenia.
What is the most likely explanation of his presentation?
- Septic shock
- Hemophagocytic lymphohistiocytosis (HLH)
- Transformation to acute myeloid leukemia (AML)
- Progression to myelofibrosis (MF)
- Transformation to small lymphocytic lymphoma (SLL)
 Medicine
Medicine
B. The accelerated phase of CHS resembles a HLH syndrome and is usually a terminal event, eventually affecting the majority of cases. It presents with massive lymphohistiocytic organ infil tration, worsening immune dysfunction and pancytopenia, increased bleeding tendency with hepato splenomegaly, and lymphadenopathy. It is thought to be precipitated by an infection with Epstein-Barr virus (EBV) that in the setting of an abnormal immune surveillance and inflammatory milieu predis poses to uncontrolled lymphoproliferation (Cancer. 1958;56(3 ):524, J Clin Immunol. 1986;6( 4):299).
need an explanation for this answer? contact us directly to get an explanation for this answer