


0
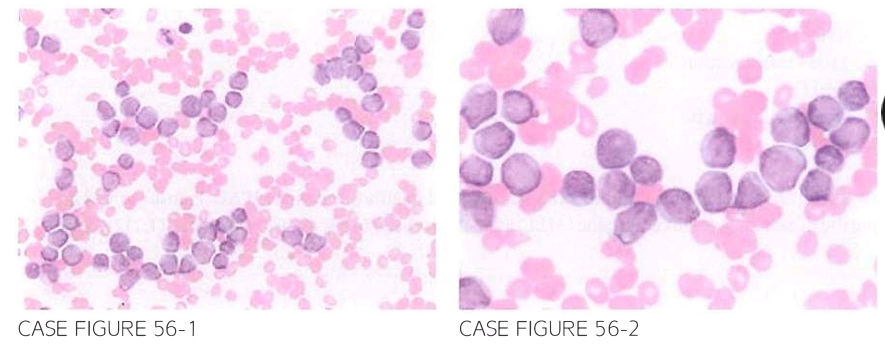
A 59-year-old female with prior history of breast cancer treated adjuvantly with doxo rubicin. cyclophosphamide. and docetaxel 3 years previously presents for further eval uation of fatigue. Patient reports that she had a normal physical examination and laboratory workup during her yearly follow-up with her primary care physician 6 months previously. Physical examination reveals pallor and petechial rash with no lymphade nopathy or hepatosplenomegaly. Laboratory workup shows leukocyte count of 133.700/,LLL. hemoglobin 7.2 g/dl. and platelet count of 8.000/,LLL. Flow cytometry reveals predominance of CD13. CD33. and CD3LJ expression. Peripheral slide is shown below.
What is the most likely cytogenetic abnormality expected in this case?
- -5
- t(9;11)
- -7
- t(l5;17)
- t(9;22)
 Medicine
Medicine
B. t-AML presenting within the first 3 years after treatment with a topoisomerase II inhibi tor (doxorubicin), and with no antecedent myelodysplastic syndrome, is most consistent with t-AML following topoisomerase II inhibitor use. The most common associated cytogenetic abnormality involves the MLL gene at chromosome llq23, and t(9;11) is the most commonly reported chromo somal abnormality. Prior exposure to radiation or alkylating agents results in t-AML that has a longer latency (5 to 7 years), is usually preceded by MDS, and is characterized by complex or monosomal karyotype (-5 or 7). Regardless of previous therapy, t-AML is associated with worse outcomes com pared with de novo cases (Br J Haematol. 2000;109(1):13, Semin Oneal. 2008;35(4):418, Blood. 2003;1 02(1 ):43 ).
need an explanation for this answer? contact us directly to get an explanation for this answer