


0
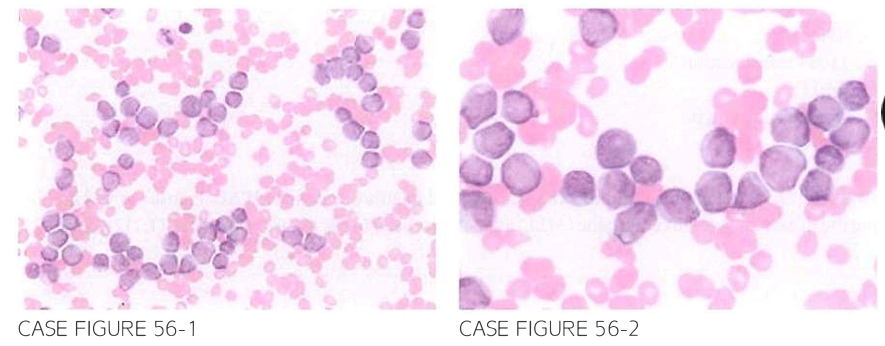
A 59-year-old female with prior history of breast cancer treated adjuvantly with doxo rubicin. cyclophosphamide. and docetaxel 3 years previously presents for further eval uation of fatigue. Patient reports that she had a normal physical examination and laboratory workup during her yearly follow-up with her primary care physician 6 months previously. Physical examination reveals pallor and petechial rash with no lymphade nopathy or hepatosplenomegaly. Laboratory workup shows leukocyte count of 133.700/,LLL. hemoglobin 7.2 g/dl. and platelet count of 8.000/,LLL. Flow cytometry reveals predominance of CD13. CD33. and CD3LJ expression. Peripheral slide is shown below.
What is the most likely diagnosis?
- Acute myeloid leukemia (AML)
- Chronic myeloid leukemia (CML)
- Myelophthisic anemia (MA)
- Acute lymphoblastic leukemia (ALL)
- Myelofibrosis (MF)
 Medicine
Medicine
A. Peripheral blood smear demonstrates leukocytes with high nuclear-to-cytoplasmic ratio, dispersed chromatin, and prominent nucleoli. This picture in addition to extreme leukocytosis and bicytopenia is most consistent with AML, specifically therapy related AML (t-AML). There is no evi dence of the typical "myeloid left shift" seen in CML cases and there is no evidence of tear drop red blood cell forms or hepatosplenomegaly as would be expected in MF. Bone marrow involvement by recurrent metastatic breast cancer causing MA might result in a leukoerythroblastic picture in periph eral blood that is not seen in this case. Flow cytometry results reveal increased expression of myeloid markers, and thus do not support the diagnosis of ALL.
need an explanation for this answer? contact us directly to get an explanation for this answer