


0
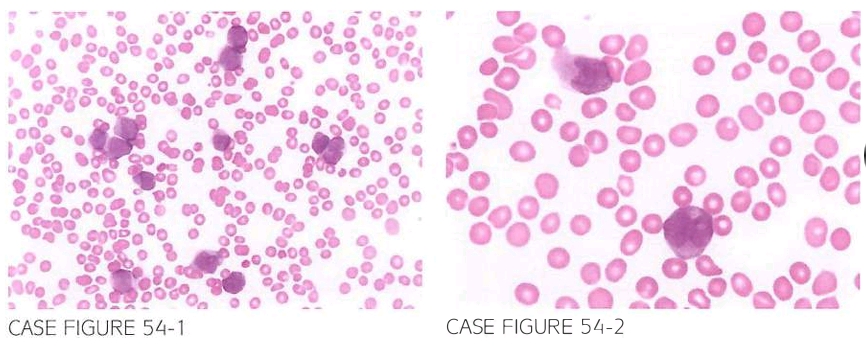
A 3LJ-year-old male is referred by his primary care physician For Further evaluation of weakness, Fatigue, and easy bruising. Physical examination reveals petechial rash. Lab oratory workup shows leukocyte count 68,200/JLL, hemoglobin 9.7 g/dl, and platelet count 6.000/ JLL. Coagulation parameters show mild prolongation of PT and PTT at 17 and LJ6 seconds. respectively. Flow cytometry reveals increased population of cells expressing CD13 and CD33, with negative expression of CD3LJ and HLA-DR. Myeloper oxidase staining is positive. Testing For nonspecific esterase is negative. Peripheral smear is shown below.
What is the most likely diagnosis?
- Acute promyelocytic leukemia (APL)
- Acute monocytic leukemia
- Acute lymphoblastic leukemia
- Burkitt leukemia
- Chronic myeloid leukemia
 Medicine
Medicine
A. Peripheral slide reveals blasts with bilobed "butterfly" nuclei and sparse or no cytoplas mic granules, which should raise suspicion for the microgranular variant of APL. Fluorescence in situ hybridization (FISH) for t(l5; 17) confirmed a diagnosis of APL. Negative staining for nonspecific esterase rules out a monocytic differentiation of these blasts. The clinical presentation with leukocyto sis, coagulopathy, lack of CD34 and HLA-DR expression, and positivity for myeloperoxidase is charac teristic of microgranular APL. This variant of APL constitutes 25% of APL cases, usually presents with leukocytosis, and is associated with a higher risk of coagulopathy, and can be confused with AML of monocytic origin; however, expression of myeloperoxidase and lack of staining for nonspecific ester ase provide a useful differentiating tool (Br J Haematol. 1982;50(2):201, Blood. 1998;91(9):3093).
need an explanation for this answer? contact us directly to get an explanation for this answer