


0
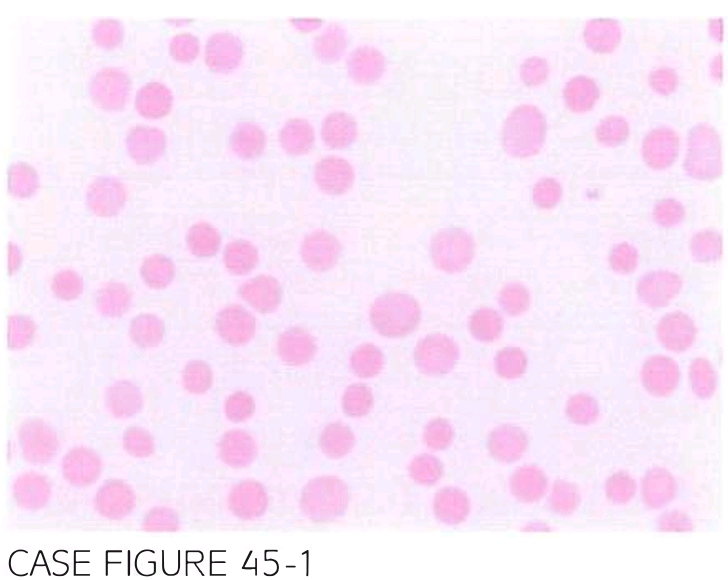
A 32-year-old Female with no known medical problems is referred For Further evalua tion of new onset anemia and thrombocytopenia. Physical examination reveals no lymphadenopathy or hepatosplenomegaly. Laboratory workup shows hemoglobin 7.6 g/dl, leukocyte count LJ,SOO/JLL, and platelet count 7,000/JLL. Direct antiglobin test is positive for lgG. LDH was elevated at 370 U/L. Testing For HIV and viral hepatitis is negative. Peripheral blood smear is shown below.
What is the most likely diagnosis?
- Evans syndrome (ES)
- Felty syndrome (FS)
- Autoimmune hemolytic anemia (AIHA)
- Immune thrombocytopenic purpura (ITP)
- Myelophthisic anemia
 Medicine
Medicine
A. Peripheral slide reveals the presence of spherocytes and reticulocytosis, which in the context of direct antiglobin test positivity and elevated LDH is consistent with the diagnosis of AIHA. There is no clear underlying etiology of thrombocytopenia, and given the presence of AIHA, it is very likely caused by immune destruction, ITP. The combination of AIHA and ITP is referred to as ES. FS is characterized by the presence of rheumatoid arthritis, neutropenia, and splenomegaly. Absence of leukoerythroblastosis in peripheral blood argues against the presence of myelophthisic anemia. ES can present as a primary disorder or occur in context of another autoimmune condition. Management fol lows the algorithm for AIHA and ITP with the use of corticosteroids, splenectomy, rituximab, or other immunosuppressive agents. The course of ES tends to be more aggressive than that of either AIHA or ITP, and is characterized by a chronic course with frequent relapses (Blood. 2009;114(15):3167, Br J Haematol. 2006;132(2):125).
need an explanation for this answer? contact us directly to get an explanation for this answer