


0
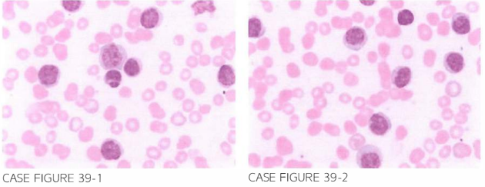
A 76-year-old male presen ts for further evaluation of dyspnea and progressive ery-thematous rash on both lower extremities. Physical examination con firms the presence of erythematous plaques on both lower extremities in addition to disclosing hepato-splenomegaly and decreased breath sounds at both lung bases. I magi ng shows bilat-eral moderate pleural effusions. Laboratory worku p reveals hemoglobin of 8.6 g/dl. leukocyte count of 1 7 3 ,000/,LLL, and platelet count of 98.000/,LLL. Flow cytometry reveals expression of CD2 , CD3 , CDLJ , CDS, CD7 , and CD52 , with lack of CDS expres- sion . Peripheral sl ide is shown below.
What is the most likely diagnosis?
- Chronic lymphocytic leukemia (CLL)
- T-cell prolymphocytic leukemia (T-PLL)
- B-cell prolymphocytic leukemia (B-PLL)
- T-cell large granular lymphocyte leukemia (T-LGL)
- Mantle cell lymphoma (MCL)
 Medicine
Medicine
B. Peripheral blood examination reveals the presence of increased number of lymphoid cells that are characteristically larger than their normal counterparts and exhibit condensed chromatin and the presence of single nucleoli in addition to increased amount of basophilic cytoplasm lacking granulation. Flow cytometry shows expression of T-cell markers, and thus rules out MCL, B-PLL, and CLL. The lack of cytoplasmic granulation argues against the diagnosis ofT-LGL. T-PLL is a rare postthymic T-cell neoplasm. Hepatoplenomegaly is a common presenting manifestation. T-PLL is known to be associated with serous effusions and skin infiltration in up to 20% of cases. Skin lesions include nodules, rash, and erythroderma. CLL is a B-cell malignancy; however, a small case series describing 25 cases of what appeared to be T-cell CLL was reported. The abnormal lymphocytes did not exhibit the typical phenotype of prolymphocytes and thus did not meet diagnostic criteria for T-PLL. Whether these cases do represent rare cases of T-CLL or nonclassical T-PLL is not entirely clear. The prognosis ofT-PLL is poor, with no clearly defined treatment regimens. Alemtuzumab and pentostatin have been used with response rates in excess of 50%; however, the duration of response is characteristically short (Blood. 1995;86(3):1 163, Mayo Clin Proe. 2005;80(12):1 660, J Clin Oneal. 2002;20(1):205, Blood. 200 1 ;98(6):1721, J Clin Oneal. 2009;27(32):5425, J Clin Oneal. 1 994;12(12): 2588, Blood. 2012;120(3):538).
need an explanation for this answer? contact us directly to get an explanation for this answer