


0
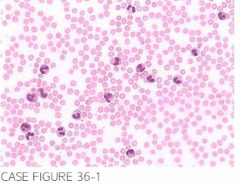
A 69-year-old male is referred by h is primary care physician for further evaluation of splenomegaly and abnormal peripheral blood coun ts. Patient reports a several-month h istory of progressive left abdominal discomfort and generalized fatigue. Physical exami nation con firms massive splenomegaly and reveals no lymphadenopathy. Labora-tory noted a leukocyte cou nt of 52 , 700/JLL, hemoglobin of 11. 3 g/d l, and platelet cou nt of 1 20,000/JLL. Peripheral blood count is shown below.
Bone marrow aspiration and biopsy revealed hypercellular bone marrow, less than 5% blasts, and no evidence of dysplasia. Testing for BCR-ABL translocation was negative.
What is the most likely diagnosis?
- Chronic lymphocytic leukemia (CLL)
- Chronic neutrophilic leukemia (CNL)
- Chronic myeloid leukemia (CML)
- Atypical chronic myeloid leukemia (aCML)
- Chronic myelomonocytic leukemia (CMML)
 Medicine
Medicine
B. Peripheral blood smear reveals increased number of mature-appearing neutrophils with blue Dohle-like inclusions and lack of less-mature myeloid forms. There is no monocytosis. Bone marrow biopsy reveals lack of dysplasia and less than 5% myeloid blasts. Testing for BCR-ABL transcript was negative. This compilation of features is characteristic of CNL. Lack of increased monocyte count does not support the diagnosis of CMML, while negativity for BCR-ABL rules out CML. Atypical CML is defined as a BCR-ABL negative myeloproliferative/myelodysplastic syndrome, and characteristically exhibits dysplastic changes. Imatinib or other tyrosine kinase inhibitors do not have activity in cases of CNL. Lasting remissions have been reported with the use of interferon alfa (Br l Haematol. 2002; 1 16( 1): 10, Curr Hematol Rep. 2004;3(3):2 10, J Clin Pathol. 2002;55(11):862, J Clin Oneal. 200 1; 19(11):29 15, Ann Oneal. 2000;1 1(4):441).
need an explanation for this answer? contact us directly to get an explanation for this answer