


0
A 58-year-old Female presents For Further evaluation of left shoulder and back pai n. Patient reports several month h istory of intermitten t skin rash and i tching. Physical exami nation reveals mild splenomegaly. Laboratory workup shows hemoglobin of 1 2 .3 g/dl, leukocyte count of 7,600/JLL, and platelet count of 1 98,000/JLL. Imagi ng of her left shoulder and spine notes several lytic lesions in the head of the humerus and diffuse osteopenia with several vertebral compression Fractures. Bone marrow biopsy is obtai ned and is shown below.
Serum tryptase levels are Found to be elevated . S taining For CD2 5 and CD 1 17 are posi tive.
What is the most likely diagnosis?
- Systemic mastocytosis
- Metastatic malignancy
- Acute myeloid leukemia with eosinophilia
- Chronic myeloid leukemia
- Myelofibrosis
 Medicine
Medicine
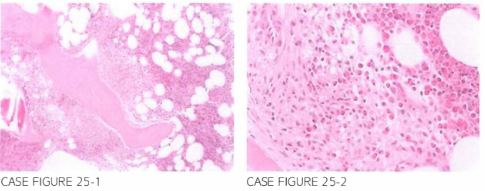
A. Bone marrow biopsy reveals a paratrabecular infiltrate by spindle-shaped hypergranular cells with irregular nuclei. Clusters of eosinophils are concentrated at the periphery of the infiltrate. Positivity for CD25 and CD 1 17 in addition to elevated tryptase levels is characteristic of mastocytosis. Diffuse musculoskeletal pain, osteopenia, and osteoporosis are associated with systemic mastocyto-sis. Serum tryptase level and staining for tryptase are useful diagnostic tools. Mutations in KIT (CD117) are detected in more than 90% of cases, and D816V mutation in KIT is the most common.
Imatinib does not have clinical activity against D816V mutant KIT (! Bone Miner Res. 1990;5(8):871, f Spinal Disord. 199 1 ;4(3):369, Bone. 2002;31 (5):556, NEJM. 1987;316(26):1622, Hematol Oneal Clin North Am. 2000;14(3):641, Blood. 2006;108(7):2366, Leuk Res. 2009;33(1 1):148 1, f Mol Diagn. 2006;8(4):412, f Allergy Clin Immunol. 2004; 1 14(1):3, Proc Natl Acad Sci USA. 1995;92(23):10560).
need an explanation for this answer? contact us directly to get an explanation for this answer