


0
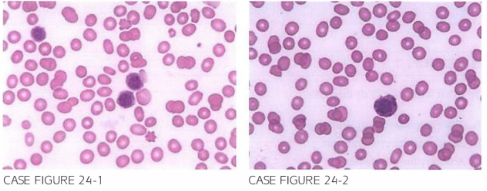
A 86-year-old female is referred for evaluation of fatigue. Physical examination reveals no lymphadenopathy or hepa tosplenomegaly. Laboratory workup shows a leukocyte count of 3 , 1 00/JLL, hemoglobin of 8 . 1 g/dl, mean corpuscular volume of 89 fl. reticulocyte count of 2.LJ%, and platelet count of 32,000/,LLL. Peripheral blood smear is shown below.
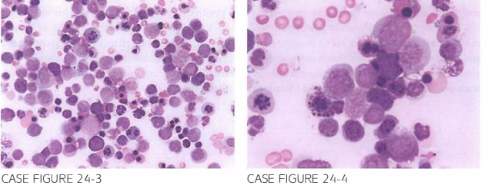
Bone marrow aspira tion is obtained and is shown below.
Flow cytometry revealed lack of CD 1 3 , CD3 3, CD3Lj, and H LA-DR expression. Myelo-peroxidase (MPO) testing returned negative while glycophori n was positive.
What is the most likely diagnosis?
- Acute megakaryoblastic leukemia
- Acute promyelocytic leukemia
- Acute erythroid leukemia
- Burkitt lymphoma in leukemia phase
- Myelofibrosis
 Medicine
Medicine
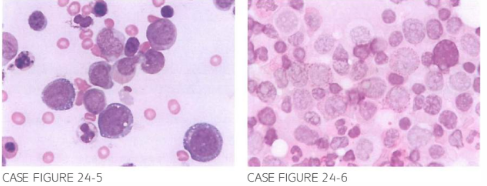
C. Peripheral blood smear exhibits the presence of abnormal cells resembling erythroid precursors, with nuclear irregularity and fragmentation. Bone marrow aspirate shows increased number of erythroid precursors exhibiting gigantism, karyorrhexis, multinucleation, and cytoplasmic and perinuclear vacuoles that are periodic-acid Schiff positive (Fig. 24-6), findings that are character-istic of acute erythroid leukemia (Di Guglielmo disease). Erythroblasts do not express myeloid lineage markers and do not stain for MPO. Positivity for glycophorin, a red blood cell membrane glycoprotein, and reaction with antihemoglobin antibodies can provide diagnostic clues. Cytoplasmic vacuoles are also seen in Burkitt lymphoma/leukemia and can result in diagnostic confusion, but the vacuoles in BL stain positive with Oil-red-O for lipid (Blood. 20 10; 1 15(10):1985).
need an explanation for this answer? contact us directly to get an explanation for this answer