


0
A 79-year-old male with no signi ficant prior medical history presen ts for further evaluation of fatigue and generalized weakness for the last several mon ths. He denies night sweats and fever. Physical examination shows no splenomegaly or lymphadenopathy. Laboratory evaluation discloses hemoglobin of 1 0. 1 g/dL. MCV of 11 0 FL. leukocyte count of 5.600/JLL. and platelet count of 1 36.000/JLL. Peripheral blood smear is shown below.
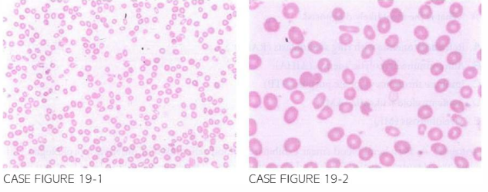
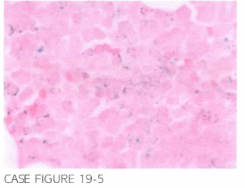
Vitamin B12 and folate levels are normal. Patient den ied alcohol use. Bone marrow biopsy is obtai ned and shows a hypercellular bone marrow. Sample of bone marrow aspirate in addition to a Prussian blue-s tai ned specimen are shown below.

What is the most likely diagnosis?
- Refractory anemia with ring sideroblasts (RARS)
- Autoimmune hemolytic anemia (AIHA)
- Immune thrombocytopenic purpura (ITP)
- Acute myeloid leukemia (AML)
- Myelofibrosis (MF)
 Medicine
Medicine
A. Peripheral blood smear exhibits red blood cells (RBC) of different morphologies with ovalocytes, teardrop-shaped RBCs, and few acanthocytes. There also appears to be at least two differ-ent red blood cell populations, one that is more normal appearing and the other with hypochromia and anisopoikilocytosis. Bone marrow sample reveals evidence of dysplastic erythropoiesis, nuclear bud-ding and cytoplastic vacuoles in RBC precursors, defective granulation of myeloid progenitors, and increased ring sideroblasts. There is no evidence of bone marrow fibrosis. This clinical presentation is most consistent with RARS. It has been recently reported that SF3Bl haploinsufficiency leads to ring sideroblast formation in patients with myelodysplastic syndromes (Blood. 20 12;120:73-3 1 86, Blood. 1982;59(2):293).
need an explanation for this answer? contact us directly to get an explanation for this answer