


A 67-year-old male is referred by h is primary care physician for further evaluation of elevated hemoglobi n level. Patien t reports feeling generally wel l; however. on review of systems. he does report mild fatigue and left abdominal discomfort. Patien t is a non-smoker with no h istory of cardiac or pulmonary disease. Exami nation reveals a male with a ruddy complexion and splenomegaly. Laboratory workup shows hemoglobin of 1 9 .5 g/dl. mean corpuscu lar volume 79 FL. leukocyte count of 1 9 .800/JLL. and plate-let count of 3 56.000/JLL. Peripheral blood smear shows no gross abnormalities. Testing for JAK2 V6 1 7 F mutation is instead of returned positive. and patien t is diagnosed with polycythemia vera (PV) .
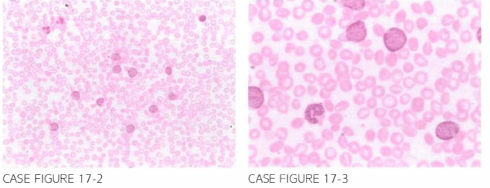
After a period of 3 more years . the patien t presen ts to the emergency department com plaining of fatigue and dyspnea on exertion . Physical examina tion reveals petech iae on both lower extremities. Laboratory evaluation reveals a hemoglobin o 7.6 g/dl, leukocyte count of 36.200/fLL, and platelet count of 22.000/fLl. Peripheral blood smear is shown below.
What is the most likely diagnosis?
- Progression to acute leukemia
- Aplastic anemia
- Transformation to chronic myeloid leukemia
- Immune thrombocytopenic purpura
- Autoimmune hemolytic anemia
 Medicine
Medicine
A. Peripheral blood smear reveals large leukocytes with high nuclear-to-cytoplasmic ratio with fine chromatin consistent with blasts. Flow cytometry was positive for CD 13 and CD33 while myeloperoxidase stain was positive confirming the diagnosis of acute myeloid leukemia. Transforma-tion to acute leukemia has been reported in less than 5% of cases of post-PV or primary myelofibrosis (Blood. 2005;1 05(3):973, Blood. 2005;1 05(7):2664).
need an explanation for this answer? contact us directly to get an explanation for this answer