


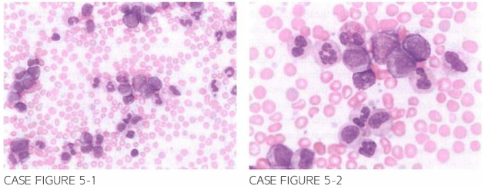
A 6 6-year-old female previously heal thy presen ts for further evaluation of diffuse bone pai n. left-sided abdomi nal discomfort. and progressive fatigue for the last several mon ths. Examination is sign i ficant for splenomegaly, easily palpable below the left costal margin extending to the m idline. Laboratory evaluation reveals leukocyte count of 1 67.000/,LLL. hemoglobi n 9.2 g/dl. and platelet count of 730.000/JLL. Peripheral blood smear is shown.
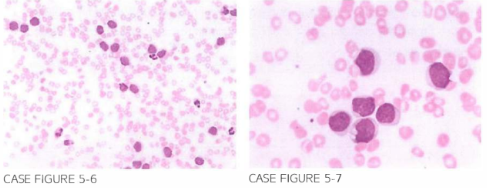
l matinib is temporari ly discontinued. and the patien t is treated with diuretics . l matinib is rei n troduced with no further recurrence of periorbital edema. Patien t con tinues on i matinib for the next 3 years and achieves complete molecular response by 18 months. However. LJ6 months after initiation of therapy. she presen ts complaining of several months of worsen ing fatigue. left-sided abdominal pai n. and nigh t sweats . Patien t re-ports adherence to imatinib regimen. Evaluation reveals leukocyte coun t of 1 2 5 .000/,LLL. hemoglobin 8.2 g/dl. and platelet count of 80.000/,LLL. Peripheral blood smear is shown below.
What is the most likely explanation of her presentation?
- Imatinib toxicity
- Transformation to chronic lymphocytic leukemia
- Progression to acute myeloid leukemia
- Development of myelofibrosis
- Noncompliance with imatinib
 Medicine
Medicine
C. Medication noncompliance should always be considered in the differential diagnosis of a CML patient with suboptimal response or loss of response to therapy. However, in this case patient reports adherence to her regimen, which makes this a less likely etiology. Peripheral smear reveals predominance of a uniform cell population with increased nuclear-to-cytoplasmic ratio with fine chromatin consistent with myeloblasts. Bone marrow aspirate showed 64% myeloblasts. This picture is diagnostic of progression to AML.
need an explanation for this answer? contact us directly to get an explanation for this answer