


0
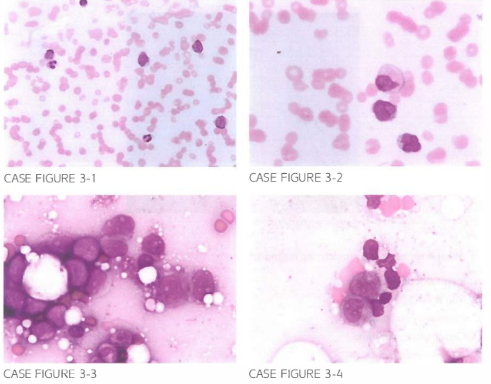
A LJ8-year-old male presen ts to the emergency room for further evaluation of a 3-week history of progressively worsening Fatigue. Physical examination reveals pal lor and dif-Fuse petech iae over lower extremities. Laboratory evaluation shows a total leukocyte cou nt of 2 3, LJOO/,uL. hemoglobin 9.8 g/dl. and platelet count of 1 3, 000/,uL. Periph-eral blood smear and bone marrow aspirate are shown.
Patient achieved a complete remission following induction chemotherapy. What is the most ap-propriate management following achievement of complete remission?
- Observation
- Refer for autologous HSCT
- Refer for allogeneic HSCT
- Consolidation with high-dose cytarabine
- Consolidation with 5 days of cytarabine with 2 days of daunorubicin
 Medicine
Medicine
D. Patients younger than 60 years of age with favorable cytogenetic profile appear to derive survival benefit from repeated cycles of high-dose cytarabine consolidation. There does not appear to be benefit for allogeneic HSCT in first remission in such patient population. Contrastingly, high-risk patients should be referred for allogeneic HSCT after achieving first remission. There is no role for autologous HSCT in the management of AML (N Engl J Med. 1994;33 1 (14):896, lAMA.
2009;301(22):2349, Cancer. 2005;103(8):1652).
need an explanation for this answer? contact us directly to get an explanation for this answer