


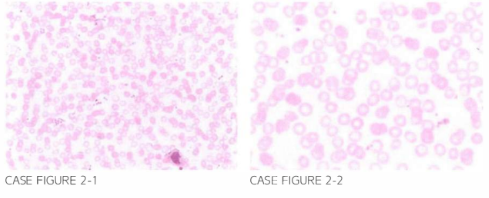
A 2 1 -year-old African American male is referred by h is primary care physician for fur-ther evalua tion of anemia. Patien t den ies his tory of melena or hematochezia. There is no prior history of episodic bone pain or family h istory of blood disorders. Physical examination reveals a young male with no hepatosplenomegaly. Labora tory workup reveals a total leukocyte count of 6.500/,uL. hemoglobin 7 .2 g/d L. mean corpuscular volume (MCV) 67 FL. red blood cell count of 2 .2 mill ion/ ,uL. and platelet count of 280.000/ p l. Peripheral blood smear is shown below.
On further ques tioni ng, the patien t reported several month history of hemoptysis; however. he den ied hematuria. epistaxis. or a sore throat. Chest x-ray revealed bilateral intersti tial and hilar infil trates (shown below) . Urine analysis showed m icroscopic he-maturia. Lung biopsy was obtai ned with evidence of hemosideri n-laden macrophages.

What is the most likely underlying diagnosis?
- Streptococcal pneumonia
- Mitral valve prolapse
- Pulmonary embolism
- Goodpasture syndrome
- Wegener granulomatosis
 Medicine
Medicine
D. Goodpasture syndrome is associated with pulmonary vasculitis and nephritic syndrome. It is caused by pathologic autoantibodies directed against collagen type IV in the glomerular basement membrane as well as pulmonary vasculature. Wegener granulomatosis is associated with involvement of the upper respiratory tracts in addition to pulmonary and renal vasculature. Antineutrophil cyto-plasmic antibodies directed against proteinase 3 are typically detected in Wegener granulomatosis (Ann Intern Med. 1996;124(7):65 1).
need an explanation for this answer? contact us directly to get an explanation for this answer