


0
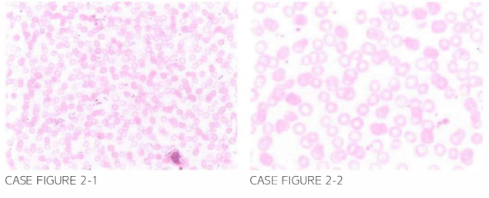
A 2 1 -year-old African American male is referred by h is primary care physician for fur-ther evalua tion of anemia. Patien t den ies his tory of melena or hematochezia. There is no prior history of episodic bone pain or family h istory of blood disorders. Physical examination reveals a young male with no hepatosplenomegaly. Labora tory workup reveals a total leukocyte count of 6.500/,uL. hemoglobin 7 .2 g/d L. mean corpuscular volume (MCV) 67 FL. red blood cell count of 2 .2 mill ion/ ,uL. and platelet count of 280.000/ p l. Peripheral blood smear is shown below.
What is the most likely diagnosis?
- Beta thalassemia major
- Alpha thalassemia trait
- Iron-deficiency anemia
- Beta sickle cell thalassemia
- Beta thalassemia intermedia
 Medicine
Medicine
C. The blood smear shows microcytic hypochromic red cells without basophilic stippling.
Iron-deficiency anemia is characterized by microcytic hypochromic red blood cells. Microcytosis would be expected in beta thalassemia intermedia or major as well as in alpha thalassemia trait However, a decreased red blood cell count is more consistent with iron deficiency, as thalassemic dis-orders typically present with microcytic polycythemia, and basophilic stippling may be seen in the red cells. In addition to iron deficiency and thalassemic disorders including hemoglobin C, D, and E dis-eases, differential diagnosis of microcytic anemia includes anemia of chronic disease, congenital sid-eroblastic anemia, lead poisoning, aluminum toxicity associated with dialysis, copper deficiency, zinc excess, and hereditary pyropoikilocytosis. Iron deficiency is always a manifestation of an underlying pathologic process, and evaluation should always proceed to uncover the underlying disease entity.
need an explanation for this answer? contact us directly to get an explanation for this answer