


A 7 LJ-year-old male with no sign i ficant medical history is referred by h is primary care physician For Further evaluation of generalized lymphadenopathy. Patient reports no preceding weigh t loss. n igh t sweats. or Fever. On physical examination. lymphade-nopathy and splenomegaly are Found. with the spleen edge pal pable 7 em below the left costal margi n. Laboratory workup reveals a total leu kocyte count of 36.500/pl. with the majority of cells of the type shown below. hemoglobin 1 LJ.S g/dl and a plate-let count of 3LJ2 .000/ pl.

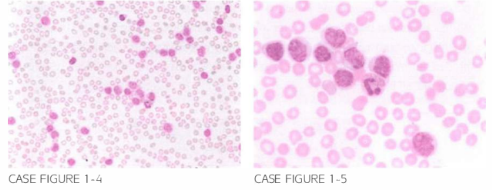
Patien t was appropriately treated for cryptococcal meni ngitis with resolution of neu-rological symptoms. However. 18 months after completion of in i tial therapy, patien t presen ted wi th recu rrence of nigh t sweats and 1 5-pound weigh t loss. Labora tory eval-uation revealed a lymphocyte count of 1 1 2 .000/,LLL. Peripheral blood smear is shown below.
What is the most likely explanation for his clinical presentation?
- Transformation to acute lymphoblastic leukemia
- Prolymphocytic transformation
- Richter syndrome
- Disseminated cryptococcal infection
- Fludarabine-induced myelodysplastic syndrome
 Medicine
Medicine
B. Peripheral slide reveals a combination of the typical small lymphocytes characteristic of CLL, in addition to larger lymphocytes, with a prominent single nucleolus, less condensed chromatin, and more abundant cytoplasm. Clinical presentation is most consistent with prolymphocytic transfor-mation, which develops in 10% of CLL cases and usually represents a terminal event secondary to re-sistance to usual chemotherapeutic agents. Richter transformation occurs in less than 10% of cases and refers to progression to an aggressive form of NHL (Cancer. 198 1;48(1 1):2447, Br J Haematol. 1986;64(1):77).
need an explanation for this answer? contact us directly to get an explanation for this answer