


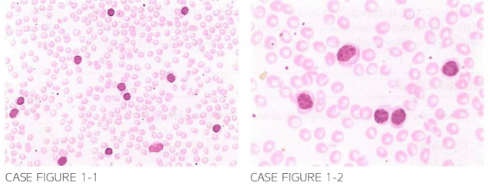
A 7 LJ-year-old male with no sign i ficant medical history is referred by h is primary care physician For Further evaluation of generalized lymphadenopathy. Patient reports no preceding weigh t loss. n igh t sweats. or Fever. On physical examination. lymphade-nopathy and splenomegaly are Found. with the spleen edge pal pable 7 em below the left costal margi n. Laboratory workup reveals a total leu kocyte count of 36.500/pl. with the majority of cells of the type shown below. hemoglobin 1 LJ.S g/dl and a plate-let count of 3LJ2 .000/ pl.
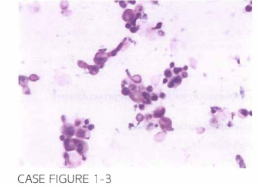
Patien t received LJ cycles of FCR with signi ficant decrease in the size of lymph nodes ,normal ization of lymphocyte count, and disappearance of B symptoms. Five months after completion of therapy, patient p resen ted to the emergen cy departmen t com-plaining of subacute change in h is mental status. Complete blood cou nt revealed normal peripheral b lood coun ts. After a negative computed tomography (CT) scan of the head, cerebrospi nal fl uid (CSF) analysis was performed wi th increased levels of protein, normal gl ucose levels, and increased lymphocyte coun ts. Microscopic exami-nation of CSF is shown below.
What is the most likely diagnosis based on the clinical presentation and CSF examination?
- Meningeal leukemia
- Hyperleukocytosis
- Cryptococcal meningitis
- Cerebrovascular accident
- Streptococcal meningitis
 Medicine
Medicine
C. Cryptococcal organisms are noted in the CSF as translucent "soap bubbles" among an inflammatory infiltrate, and stain positive with India ink. Antigen testing for Cryptococcus was also positive. Fludarabine-induced lymphopenia increases the risk of opportunistic infections, and prophy-lactic anti-infective agents should be considered during, and for several months after, completion of fludarabine-based therapy (Am J Hematol. 1995;49(2): 1 35).
need an explanation for this answer? contact us directly to get an explanation for this answer