


History
A 37-year-old woman attends the antenatal clinic at 18 weeks’ gestation. She is gravida 2 para 1, having had a spontaneous vaginal delivery at term 8 years ago. This current pregnancy was achieved through in vitro fertilization after four attempts (cycles). Two embryos were implanted. The first-trimester scan confirmed a twin gestation and noted a lambda sign between the gestations sacs. The anomaly scan is due in 2 weeks. So far the woman has been feeling nauseated and tired but well.
Examination
The blood pressure is 120/78 mmHg. The fundus is palpable 2 cm above the umbilicus. Two separate fetal hearts are heard on hand-held fetal Doppler, one 143/min, the other 130/min.
Questions
• How would you interpret the results?
• What can the parents be told about the zygosity of the pregnancy?
• How would you monitor and manage this pregnancy?
 Medicine
Medicine
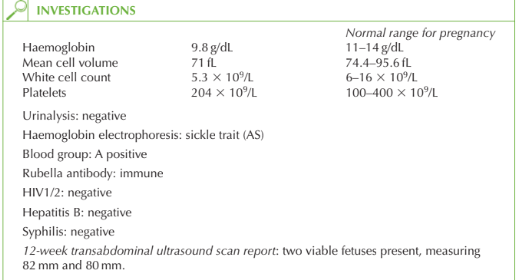
The ultrasound confirms a twin pregnancy with a lambda sign (projection of placental tis-sue between the dividing membranes). This is suggestive of a dichorionic pregnancy. The woman is anaemic with a low mean cell volume suggestive of iron-deficiency anaemia. The only other investigation of note is that the woman has sickle trait. Zygosity Although the pregnancy appears dichorionic diamniotic (DCDA), this does not inform us about zygosity. A monozygotic pregnancy may be DCDA if the embryo has split at an early stage. One third of monozygotic pregnancies are DCDA, two-thirds monochorionic diamni-otic and around 1 per cent are monochorionic monoamniotic. Confirmation of zygosity is with placental histology, or by observing that the fetuses are of different genders.
Monitoring
Twin pregnancies are associated with increased maternal risks of hyperemesis, anaemia, preterm labour, antepartum haemorrhage, pre-eclampsia, gestational diabetes, thrombosis and Caesarean delivery. The fetuses are at risk of intrauterine growth restriction, prematurity, stillbirth or neonatal death, congenital anomalies and operative delivery.
Management
In addition to routine antenatal care this woman needs:
• information regarding the increased maternal and fetal risks with twin pregnancy
• regular hospital antenatal assessment from the late second trimester
• ferrous sulphate and folic acid supplementation
• discussion of mode of delivery (depending on growth and presentation of twins at around 36 weeks)
• hospital delivery by 40 weeks
• introduction to multiple pregnancy support groups.
The woman has sickle trait and her partner should also be tested. If he is also sickle trait positive then prenatal testing of the babies should be offered to determine whether they are homozygous and therefore going to be affected by sickle cell disease.
KEY POINTS
• Chorionicity and amnionicity can be determined with high accuracy by ultrasound in the first trimester but, unless the fetuses are seen to be of different sexes, the zygosity of dichorionic diamniotic twins can only be confirmed with genetic or histological testing.
• Multiple pregnancies are high risk for both mother and babies, and close monitoring is essential for the early detection of problems.
• A woman with sickle cell trait whose partner is also sickle cell trait positive should be offered prenatal diagnosis by chorionic villus sampling, amniocentesis or cordocentesis.
need an explanation for this answer? contact us directly to get an explanation for this answer