


History
A woman attends the antenatal day assessment unit to discuss the result of her glucose tolerance test. She is 42 years old and this is her sixth pregnancy. She has previously had three Caesarean sections, one early miscarriage and a termination of pregnancy. All book-ing tests were normal as were her 11–14-week and anomaly ultrasound scans.
The woman is of Indian ethnic origin but was born and has always lived in the UK. She is now 26 weeks’ gestation and her midwife arranged a glucose tolerance test because of a family history of type 2 diabetes (her father and paternal aunt).
Examination
The body mass index (BMI) is 31 kg/m2. Blood pressure is 146/87 mmHg. The symphysio-fundal height is 29 cm and the fetal heart rate is normal on auscultation.
Questions
• What is the diagnosis and on what criteria can this be made?
• What are the principles of management for this patient?
 Medicine
Medicine
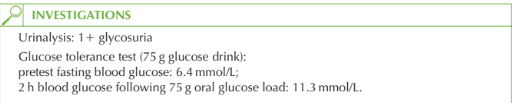
The diagnosis is of gestational diabetes mellitus (GDM) and is based on the 2 h glucose concentration exceeding 11.1 mmol/L (World Health Organization (WHO) criteria). The diagnosis may also be made if the fasting blood glucose exceeds 7.8 mmol/L, in which case a formal glucose tolerance test would not have been necessary. Transient glycosuria is common in pregnancy and may occur after a glucose-rich drink or snack. Therefore the urinalysis alone is unhelpful in the assessment of this woman. GDM occurs in up to 3 per cent of the pregnant population depending on the ethnic diver- sity of the specific population. In some cases it may be the first presentation of previously undiagnosed diabetes.
The importance of the diagnosis relates to the effect on the mother and fetus.
• Effects on the fetus:
• fetal macrosomia
• polyhydramnios
• neonatal hypoglycaemia
• neonatal respiratory distress syndrome
• increased stillbirth rate
• Effects on the mother:
• increased risk of traumatic delivery (e.g. shoulder dystocia)
• increased Caesarean section risk
• increased risk of developing GDM in subsequent pregnancies
• 50 per cent increased risk of developing type 2 diabetes within 15 years Management principles
• Optimal control of maternal blood glucose minimizes the chance of fetal compli-cations. This needs the multidisciplinary input of a diabetologist, specialist diabetes nurse, dietitian, specialist midwife and obstetrician.
• Dietary advice and counselling are the initial interventions (reduced fat and carbo-hydrate intake with weight control).
• Blood glucose monitoring at home should be initiated with pre- and post-prandial levels at each meal.
• Oral hypoglycaemics are contraindicated in pregnancy.
• If blood glucose measurements are repeatedly high, insulin should be commenced.
• The fetus should be monitored with regular ultrasound scans for growth and liquor volume (polyhydramnios being a sign of fetal polyuria secondary to excessive glucose level).
• Delivery should be planned by 40 weeks, but Caesarean section should be performed for obstetric indications only.
• Sliding-scale insulin should be initiated in labour for women on insulin.
• The insulin can be stopped immediately postpartum as normal glucose homeostasis returns rapidly after delivery.
• The fetus should be carefully monitored for neonatal hypoglycaemia.
• The mother should have a repeat glucose tolerance test 6 weeks postpartum to rule out pre-existing diabetes.
KEY POINTS
• Gestational diabetes should initially be treated with dietary and weight advice. Insulin may be needed if blood glucose levels remain high.
• One-third of women with impaired glucose tolerance in pregnancy will go on to develop diabetes mellitus in the next 25 years.
need an explanation for this answer? contact us directly to get an explanation for this answer