


History
A 31-year-old woman presents with vaginal bleeding at 5 weeks 6 days’ gestation. She has had a previous left uterine tubal ectopic pregnancy managed with laparoscopic sal-pingectomy. She is certain of her last menstrual period date and has regular cycles. Her last smear test was normal and she has not used contraception since her last pregnancy 3 years ago.
When she was 21 years she had an episode of pelvic inflammatory disease treated with intravenous antibiotics. She is otherwise not aware of having had any sexually transmit-ted infections. She has been with her partner for 7 years. She smokes 10 cigarettes per day and does not drink alcohol. The bleeding is described as very light and she has not been aware of any pain. She has not felt dizzy or lightheaded and has no shoulder-tip pain.
Examination
She is warm and well perfused. The blood pressure is 136/78 mmHg and heart rate 75/min. The abdomen is not distended and no tenderness is elicited on palpation. The cervix is closed. The uterus feels normal size, anteverted and mobile, and there is no cervical exci-tation. Gentle adnexal examination shows no significant tenderness.
Questions
• What is the diagnosis?
• What management options are available and which management would be pre-ferred in this particular case?
 Medicine
Medicine
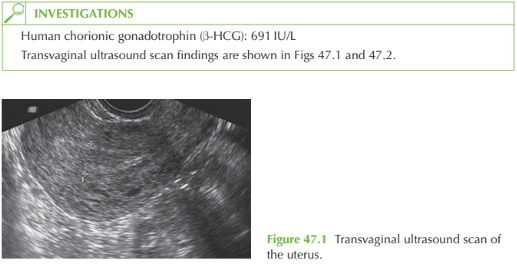
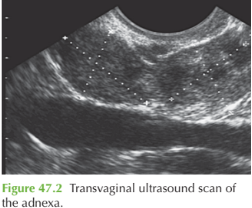
The ultrasound scan shows an empty uterus and an adnexal mass adjacent to the right ovary. The mass represents an ectopic pregnancy. No gestation sac or fetal pole is visible and the pregnancy is therefore not considered ‘viable’. However there is still a possibility of rupture if not treated.
Management
Three options might be appropriate to this woman:
• surgical: laparoscopic excision of the tube (salpingectomy) or salpingotomy to incise the tube and flush out the ectopic pregnancy
• medical: intramuscular methotrexate to destroy the rapidly dividing trophoblast tissue, with regular HCG follow-up to confirm resolution
• expectant: ‘wait and see’ approach, suitable if the HCG at 48 h is decreasing spontaneously and the woman remains asymptomatic.
In this case the woman has previously had a uterine tube removed and surgery might compromise the remaining tube, so methotrexate treatment is preferred. However if the tube is damaged but preserved, she may be at high risk of further ectopic pregnancy. Prerequisites for methotrexate are normal full blood count, renal and liver function before treatment, compliance with the intense follow-up, and understanding the need not to become pregnant again for at least 3 months due to the potential teratogenic effects. Potential side-effects are abdominal pain (sometimes difficult to distinguish from pain suggestive of tubal rupture), nausea, diarrhoea and, rarely, conjunctivitis and stomatitis.
KEY POINTS
• Ectopic pregnancies are commonly asymptomatic or associated with atypical symptoms.
• Surgical, medical or expectant management of ectopic pregnancy depend on the symptoms, signs and HCG result.
• Methotrexate is effective but follow-up is intensive and sometimes prolonged.
need an explanation for this answer? contact us directly to get an explanation for this answer