


History
A 24-year-old woman presents with the absence of periods for 9 months. She started her nperiods at the age of 13 years and had a regular 28-day cycle until 18 months ago. The periods then became irregular, occurring every 2–3 months until they stopped completely. She has also had headaches for the last few months and is not sure if this is related. She has a regular sexual partner and uses condoms for contraception. She has never been pregnant. There is no previous medical history of note. She works as a primary school teacher and drinks approximately 4 units of alcohol per week. She does not smoke or use recreational drugs. She jogs and swims in her spare time.
Examination
The woman is of average build. The blood pressure and general observations are normal. The abdomen is soft and non-tender and speculum and bimanual examination are unremarkable.
Questions
• What is the diagnosis?
• Are any further investigations indicated?
• How would you manage this patient?
 Medicine
Medicine
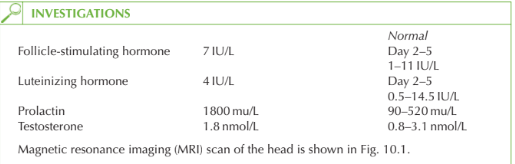
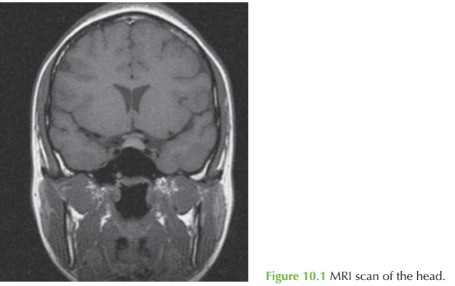
The investigations show a high-prolactin and a space-occupying lesion in the pituitary fossa in the region of the anterior pituitary as detailed in Figure 10.2. This is consistent with a pituitary adenoma (prolactinoma).
Prolactin should always be measured in a woman with amenorrhoea. Care should be taken in interpreting the results, as levels up to 1000 mu/L can be found as a result of stress (even due to venepuncture), breast examination or in association with polycystic ovarian syndrome). Above 1000 mu/L the usual cause is a pituitary adenoma (micro- or macroscopic).
Further investigation Visual fields should be checked, as visual field defects may be present with a large tumour. The other important investigation in any woman with amenorrhoea is a pregnancy test, although with this history this would be very unlikely. (Prolactin is also raised in pregnancy.)
Management
Most prolactinomas respond to medical treatment with bromocriptine or cabergoline. Maintaining the prolactin level below 1000 mu/L causes menstruation (and ovulation) to return in most women. This can be continued indefinitely or until pregnancy is achieved if the presenting complaint is of infertility.
KEY POINTS
• Hyperprolactinaemia is a common cause of secondary amenorrhoea.
• Prolactin levels up to 1000 u/L may be due to non-pathological causes such as stress.
• Prolactinomas can usually be treated with medical suppression, and surgery is only indicated rarely.
need an explanation for this answer? contact us directly to get an explanation for this answer