


0
History
A 39-year-old woman is referred from the haematologist, with anaemia. She had been complaining of increasing tiredness and shortness of breath for 3 months, with frequent headaches.
Her periods occur every 24 days and the first day is generally moderate but the second to fourth days are very heavy. She uses tampons and sanitary towels together. She has no pain. Her last smear test was normal 2 years ago. She had no previous gynaecological problems and takes no medication.
Examination
The woman is slim with pale conjunctivae. Abdominal, bimanual and speculum examin-ation are unremarkable.
Questions
• How do you interpret these findings?
• What is the likely underlying diagnosis?
• How would you manage this woman?
 Medicine
Medicine
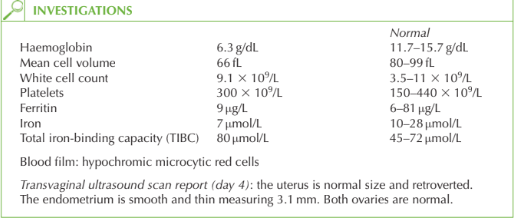
The blood count shows anaemia with reduced mean cell corpuscular volume and low mean cell haemoglobin suggestive of a microcytic anaemia. Iron deficiency is the com-monest cause for this picture and is confirmed by the low ferritin and iron, with raised iron-binding capacity. The anaemia accounts for the breathlessness, tiredness and headaches.
Menorrhagia is the commonest cause of anaemia in women, and in this case is supported by the history of excessive bleeding. The woman herself may not recognize that her periods are particularly heavy if she has always experienced heavy periods or if she thinks it is normal for periods to become heavier as she gets older. As no other cause of heavy bleeding is apparent from the history and the ultrasound is normal, then the underlying diagnosis is one of exclusion referred to as dysfunctional uterine bleeding (DUB).
Management
The anaemia should be treated with ferrous sulphate 200 mg twice daily until haemoglobin and ferritin are normal. It may take 3–6 months for iron stores to be fully replenished. Tranexamic acid (an antifibrinolytic) should be given during menstruation to reduce the amount of bleeding. It is contraindicated with a history of thromboembolic disease. The levonorgestrel-releasing intrauterine device is used for its action on the endometrium to reduce menorrhagia, often causing amenorrhoea, though it is commonly associated with irregular bleeding for the first 3 months. The combined oral contraceptive pill is effective for menorrhagia in young women (below 35 years).
If these first-line management options are ineffective then endometrial ablation should be considered, which destroys the endometrium down to the basal layer. It is successful in 80–85 per cent of women and they should have completed their family and use effective contraception. Hysterectomy is considered a ‘last resort’ for DUB, due to the associated morbidity.
KEY POINTS
• A woman’s perception of bleeding is not always proportionate to the actual volume lost, so haemoglobin should be checked in any woman suspected of menorrhagia.
• DUB is a diagnosis of exclusion.
• A hierarchy of first-, second- and third-line treatment should be used in management.
need an explanation for this answer? contact us directly to get an explanation for this answer