


History
A 59-year-old woman presents with a gradually worsening eruption over 7 weeks. The eruption is pruritic and has not responded to the application of emollients and moderately potent topical glucocorticoids. She has no previous history of skin lesions and reports that she is otherwise well, although she has a poor appetite and has lost 8 kg body weight over the past three months. She does not take medication. She works as a shop assistant and consumes 10 units of alcohol per week. She stopped smoking four years ago.
Examination
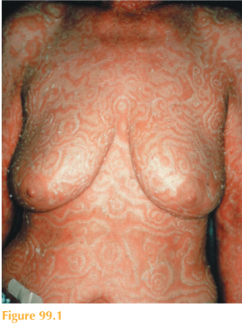
The patient’s pulse is 76/min and blood pressure 128/76 mmHg. Her striking skin eruption involves the trunk, limbs and neck. There are widespread macular erythematous bands with a wood-grain–like and whorled concentric configuration and fine scaling along the borders (Fig. 99.1). There are no abnormalities on examination of her cardiovascular and respiratory systems. Her abdomen is soft and non-tender with no masses palpable. She has no breast masses. She has a firm 1.5 2.0-cm left supraclavicular lymph node.
Questions
• What is this eruption?
• Is there a differential diagnosis?
• What further investigations would you perform?
• What is the management of this patient?
 Medicine
Medicine
The very striking appearance of this eruption is pathognomonic of erythema gyratum repens (EGR) and potentially a paraneoplastic process. Approximately 80 per cent of patients with EGR have an underlying malignancy. It can also be associated with con-nective tissue disease (CREST, systemic lupus erythematosus) or infection (such as tuberculosis). The characteristic concentric erythematous bands forming a wood-grain appearance help distinguish EGR from other figurate erythemas, such as erythema annu- lare centrifugum (may also be paraneoplastic or associated with drugs or other systemic illnesses), erythema migrans (associated with Lyme disease), and erythema marginatum rheumaticum (occurring in association with rheumatic fever). EGR does not respond to skin targeted therapy but rather to treatments aimed at underlying disease.
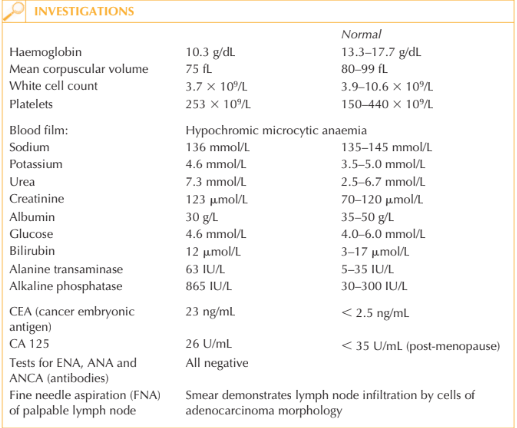
This clinical picture is highly suggestive of an underlying malignancy. The palpable left supraclavicular lymph node (Virchow’s node) with FNA findings of adenocarcinoma points towards gastric pathology.
The next investigations for this patient are an oesophago-gastro-doudenoscopy (OGD) and CT scans of the chest and abdomen. These investigations demonstrated a polypoid gastric adenocarcinoma with lymph node involvement. Resection of the malignancy and lymph node dissection resulted in rapid resolution of the skin eruption.
KEY POINTS
• The striking configuration of the erythema is pathognomonic of erythema gyratum repens (EGR).
• EGR is frequently a paraneoplastic process.
• Patients presenting with this eruption should be investigated for underlying systemic disease and in particular malignancy.
need an explanation for this answer? contact us directly to get an explanation for this answer