


History
A 15-year-old girl presents with a 3-month history of hair loss. The girl’s mother had noticed an initial small patch of hair loss over the posterior scalp. Her family had thought this might be due to ‘stress’ as the girl’s grandfather had recently died. Subsequently, the initial patch increased in size and over the past six weeks multiple patches of hair loss have been noticed. She has a past history of eczema and hay fever. She is otherwise well and has a family history of hypothyroidism.
Examination
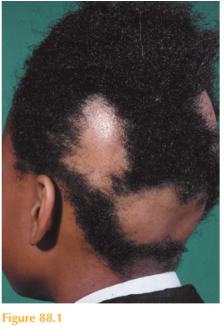
There are multiple patches of alopecia over the occipital and parietal scalp, the skin looks normal (Fig. 88.1). At the periphery of the patches of alopecia are ‘exclamation mark’ hairs. No erythema or scale is seen on the scalp. The rest of her body hair is normal, as are her nails. There is no occipital lymphadenopathy.
Questions
• What is the diagnosis?
• Would you request any investigations?
• How would you manage this patient?
 Medicine
Medicine
When assessing patients with hair loss it is important to first establish whether the alo-pecia is focal or diffuse, whether the skin on the scalp is normal or diseased and, if the skin is diseased, is there scarring? This girl had patchy alopecia with normal skin, which is highly suggestive of the diagnosis of alopecia areata. This is an autoimmune disease; inflammatory cells target the growing hairs, which subsequently fall out.
Hair growth is cyclical, with three phases: anagen (growing phase); catagen (resting phase); and telogen (shedding phase). Alopecia areata is a common autoimmune disease that occurs in approximately 1 per cent of the population and generally begins in young adults.
Classically, it presents with well-demarcated circular patches of gradual, asymptomatic hair loss with no evidence of inflammation or scarring over the scalp. Pathognomonic exclamation mark hairs are seen which appear as broken off stubby hairs due to the proximal shaft being narrower than the distal shaft. Eyebrows, eyelashes and the beard area are also affected. Other patterns include totalis where complete hair loss occurs over the entire scalp and universalis where hair is lost from all body sites. In addition, evidence of nail pitting can be seen. The differential diagnosis includes other causes of a non- scarring alopecia including tinea capitis, traction alopecia and trichotillomania (constant rubbing or pulling of the hair).
The course of alopecia areata is unpredictable. Spontaneous remission is common in more patchy disease. When regrowth occurs the hair is much finer and often white or grey initially. After the first episode, 30 per cent of patients regrow the hair within one year.
Recurrences are common, however. Poor prognosis is associated with prepubertal onset, occipital involvement, prolonged duration of hair loss in a given area and atopy.
Treatment is dependent on the extent. The prognosis for a solitary, small lesion is excel-lent, so no treatment may be required as spontaneous regrowth often occurs. For further focal disease, topical or intra-lesional corticosteroids can be helpful. For more extensive disease short courses of systemic corticosteroids, ciclosporin, phototherapy (psoralen–UVA) and topical immunotherapy to induce a contact sensitization with diphencyprone can be useful.
Alopecia areata is associated with other autoimmune diseases including vitiligo, Addison’s disease and thyroid disease, which is why the family history of autoimmune disease in this case is relevant. However, studies have shown a concordance rate of 55 per cent in monozygotic twins, suggesting that both genetic and environmental factors are relevant. Atopy also appears to be linked. Therefore, blood tests to rule out other underlying autoimmune diseases should be considered in patients presenting with alopecia areata.
KEY POINTS
• Hair growth is cyclical, in three phases: anagen, catagen and telogen.
• Alopecia areata can be focal or diffuse.
• ‘Exclamation mark’ hairs are pathognomonic of alopecia areata.
need an explanation for this answer? contact us directly to get an explanation for this answer