


History
A 50-year-old woman presents to the accident and emergency department with a 2-day history of painful facial swelling that was unresponsive to chlorpheniramine. She had seen her GP 1-day previously who prescribed flucloxacillin 500 mg qds; however, over the next day the pain and swelling had worsened. On direct questioning she thinks she may have been stung by an insect 3 days ago on her left cheek. The eruption is not pru-ritic. She has no known allergies.
Examination
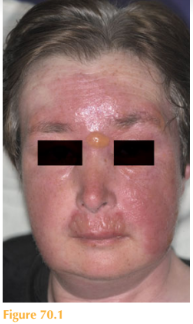
There is a well-demarcated, confluent, livid erythema with oedema and bullae formation, mainly on the left side of her face but spreading to the right (Fig. 70.1). There is no evidence of any skin erosions, no mucous membrane involvement and her vision is unaffected. She is apyrexial. Her blood pressure is 134/89 mmHg, pulse rate 92 /min, oxygen saturation on air 97%, blood sugar level on finger prick testing 7.9 mmol/L.
Questions
• What is the diagnosis?
• What is the likely underlying cause?
• What treatment would you initiate?
 Medicine
Medicine
This patient was diagnosed clinically with erysipelas. This is a cutaneous infection, usu- ally caused on the face by group A Streptococcus pyogenes, which may originate from the patient’s throat. The history of a possible insect bite was not thought to be significant but any minor skin laceration would act as a port of entry to microorganisms. The spread of the erythema is characteristically rapid and well demarcated (you could outline the edge with a skin marker); this contrasts with cellulitis, which usually has a slower onset with ill-defined margins. Cellulitis is deep, erysipelas is more superficial. Erysipelas may also affect the lower limb. The confluent erythema is very oedematous and consequently vesicles or bullae may form. The differential diagnosis of sudden-onset facial erythema includes ‘slapped cheek’ or fifth disease, however this usually occurs in children, is symmetrical, and there is little oedema and no blistering. An acute allergic reaction usually presents more rapidly over a few hours rather than days and usually results from ingesting an allergen; such patients usually have lip swelling and may have gastrointestinal upset. Patients with erysipelas should be managed initially with intravenous antibiotics. This patient was given 1.2 g benzylpenicillin and 2 g flucloxacillin qds for 2 days. The large bullae were deflated using a sterile needle. Gauze soaked in diluted potassium permanga-nate solution was applied to the affected skin once daily and topical fusidic acid applied. The patient was discharged on oral amoxicillin 1 g tds for 2 weeks.
KEY POINTS
• Erysipelas characteristically affects the face or lower limb.
• The onset or erysipelas is rapid over 48 hours with well-demarcated erythema.
• Group A Streptococcus is usually the cause and should be treated initially with intrave-nous antibiotics.
need an explanation for this answer? contact us directly to get an explanation for this answer