


0
History
An 86-year-old man presents with a bleeding lesion on his scalp. This had slowly enlarged over a 4-month period and was very painful. He had worked abroad whilst in the army 50–60 years ago. He had previously had other lesions treated on the scalp with liquid nitrogen.
Examination
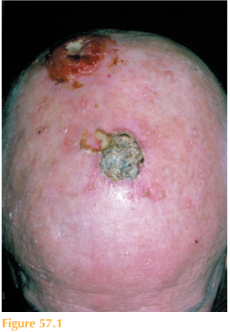
There is a large ulcerated eroded nodule over the vertex of the scalp that is friable, ery-thematous and with a soft fleshy margin (Fig. 57.1). Over the surrounding skin there are scattered erythematous patches with overlying scale. There is palpable lymphadenopathy in the cervical chain.

Questions
• What is the likely diagnosis?
• How should this patient be treated?
 Medicine
Medicine
The likely diagnosis is an invasive squamous cell carcinoma (SCC). This patient, an eld-erly man, has a friable lesion on a bald scalp, which has developed over four months.
Initially, SCCs begin as ill-defined, erythematous papules or nodules with a hyperkera-totic top (rough surface); as they enlarge they may ulcerate. He had worked in tropical climates whilst in the armed forces. The palpable cervical nodes suggest that the skin cancer may have metastasized.
The differential diagnoses would include an amelanotic malignant melanoma, and a nodular basal cell carcinoma, actinic keratoses, Bowen’s disease and a keratoacanthoma.
Invasive SCC is a malignant tumour of keratinocytes. SCCs often arise in precancerous lesions in otherwise healthy individuals over the age of 55 years. Men are more com-monly affected than women. SCCs usually arise from actinic keratoses and Bowen’s dis-ease. Actinic keratoses are single or multiple erythematous patches with adherent scale on sun-exposed skin in middle-aged adults.
Histologically, there are different levels of differentiation, which can correlate to the
aggressiveness of the SCC: well, moderately and poorly differentiated. Poorly differenti-ated lesions do not show signs of keratinization and clinically appear fleshy, friable and ulcerated as in this case. Metastasis is more common than with well-differentiated lesions.
Predisposing factors include chronic actinic damage, sites of chronic ulceration and scar-ring, exposure to ionizing radiation and immunosuppression, especially in solid organ transplant recipients and HIV disease.
Surgical excision is the treatment of choice. Depending on location and size of the lesion, it may require closure with a skin flap or graft. Mohs’ micrographic surgery may be required for difficult sites. In elderly patients, SCCs can be treated with radiotherapy if surgery is not feasible/desirable. SCCs are more aggressive than basal cell carcinomas and can metastasize. The majority of ultraviolet-induced lesions have a low rate of distant metastasis. Higher risk SCCs are defined as those on the ear, lip and genitalia. A greater incidence of metastases occurs in immunosuppressed patients. All patients with SCCs should have a full skin check to exclude any further suspicious lesions and all lymph node groups examined to exclude metastases. Suspicious nodes should be biopsied.
KEY POINTS
• Invasive squamous cell carcinoma (SCC) is a malignant tumour of keratinocytes.
• SCCs usually arise from actinic keratoses and Bowen’s disease.
• Metastases can spread into the draining lymph nodes and ultimately the blood.
need an explanation for this answer? contact us directly to get an explanation for this answer