


History
A 23-year-old African Caribbean man presents with a 2-year history of gradual patchy lightening of the skin. He denies any symptoms such as itching or irritation of his skin prior to the onset of the whitening patches. He has no previous history of skin problems but had suffered with mild asthma as a child. He is otherwise well and does not take medication. There is a family history of thyroid disease.
Examination
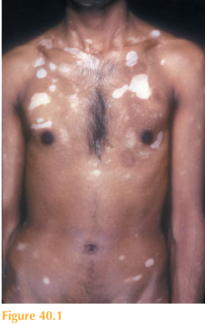
There are multiple, well-demarcated, non-scaly macules of depigmentation in a sym-metrical distribution, predominantly over the trunk (Fig. 40.1). The periorbital, perioral and genital areas are also affected. Some of the macules have tiny pigmented spots within them.
Questions
• What is the diagnosis?
• What are the different presentations of this disease?
• How should this patient be managed?
 Medicine
Medicine
This patient presented with depigmentation (leucoderma) which was asymptomatic and symmetrical. Causes of hypopigmentation include albinism, hypopituitarism, chemical leucoderma such as with phenolics, and post-inflammatory change secondary to inflam-matory dermatoses such as eczema. Onset in this patient was in adulthood (acquired) with gradual deterioration, which led to the diagnosis of vitiligo.
Vitiligo is a depigmenting acquired disease that occurs due to loss of epidermal melano- cytes. Vitiligo has been reported to be associated with autoimmune disease including thyroid disease, pernicious anaemia and type 1 diabetes mellitus. The cause of vitiligo is, however, unknown. It affects 1 per cent of the population, usually occurring between the ages of 10 and 30 years. Vitiligo affects all racial groups, but is particularly distressing in those with darker skin.
Vitiligo is characterized by sharply defined pale/white macules. Most commonly affected are periorbital, perioral and anogenital areas, but also the axillae, inguinal regions and extensor sites of the knees/elbows. Symmetrical involvement is the norm. In addition, white hair and prematurely grey hair can occur.
There are several types: a focal type which is characterized by one or more macules; segmental vitiligo occurs when the disease develops unilaterally, for instance, down one leg; generalized or universal disease can also occur. In patients with lighter skin where the contrast between disease and normal skin is less obvious, then a Wood’s light can be very helpful to evaluate the macules.
The course of vitiligo is variable; however, most patients’ course is quite rapid at the onset followed by a period of stability. Treatments are generally unsatisfactory. Photoprotective advice is essential for involved skin. Cosmetic camouflage can be useful.
To induce repigmentation, topical corticosteroids and topical calcineurin inhibitors such as tacrolimus can be effective for focal lesions. For more extensive disease phototherapy including psoralen–UVA and narrow-band UVB are effective in some patients. Response to phototherapy is usually evidenced initially by follicular repigmentation where tiny macular dots of pigmented skin are seen. In extensive disease, patients may be offered depigmentation of their remaining normal skin using monobezyl ether or hydroquinone.
KEY POINTS
• Vitiligo occurs due to loss of epidermal melanocytes.
• It has been reported to be associated with autoimmune disease.
• Focal, segmental and generalized types exist.
need an explanation for this answer? contact us directly to get an explanation for this answer