


History
A 50-year-old man presents to the on-call dermatologist with a 3-day history of rigors, feeling generally unwell and redness of all his skin associated with scaling. He also complains of swelling of his arms and legs. Since his teenage years he has suffered with a scaly scalp and occasional dry patches on the elbows. There is a family history of pso-riasis. Recently he has been experiencing increasing episodes of angina and has sought medical attention.
Examination
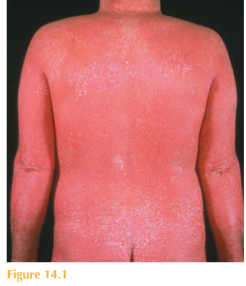
There is widespread erythema affecting the face, trunk and limbs with thickening of the skin and associated widespread scale (Fig. 14.1). Thick scale is present throughout the scalp with dystrophy of all 20 nails. Over the elbows erythematous plaques with overlying thick scale are seen. In addition there are mild bilateral ectropions.
Questions
• What is the likely diagnosis?
• What is the differential diagnosis?
• How would you manage this patient?
• What are the potential complications?
 Medicine
Medicine
The most likely diagnosis is erythrodermic psoriasis. Erythroderma is when almost the entire skin ( 90%) becomes red; in the case of psoriasis the skin is also thickened and scaly. There is usually hyperkeratosis of the palmar/plantar sites. There may be onycholy-sis (lifting of the nail plates) and even shedding of the nails. Thinning of the hair and alopecia may also occur. Clues in this patient to the underlying cause of his erythroderma are his dystrophic nails and classic plaques of psoriasis over his elbows. In addition he has a history of scalp scaling and a family history of psoriasis. Erythrodema is a serious and at times life-threatening dermatological emergency. Erythrodermic skin is associated with fever, rigors and lymphadenopathy. Other causes of erythroderma include atopic eczema, drug eruptions, cutaneous T-cell lymphoma, allergic contact dermatitis, pityriasis rubra pilaris and seborrheoic dermatitis. To diagnose the underlying cause can be very challenging and signs and symptoms of pre-existing dermatoses may help, as in this case. Complications result from significant physiological and metabolic changes that occur when the skin barrier function starts to fail. Thermoregulatory control is lost, leaving patients vulnerable to hypothermia due to excess heat loss. Dehydration commonly occurs owing to increased transepidermal water. Cutaneous inflammation may mask concurrent secondary skin infection and blood cultures may be positive owing to their easy contamination with normal skin flora. Hypoalbuminaemia and cardiac failure are serious complications that particularly affect the elderly. Treatment is supportive. In-patient management and skilled nursing care are essential. Close monitoring of pulse, blood pressure, temperature and fluid balance is mandatory. Hourly emollient therapy with liquid paraffin and mild topical steroids are the mainstay of the acute phase. The use of systemic corticosteroids in the acute setting is controver-sial, as there is some evidence they can exacerbate the condition and may even have been the initial trigger. Adequate nutritional support to minimize protein losses is important. Haemodynamic instability and intercurrent infections are treated as necessary. Patients usually require systemic therapy; historically ciclosporin has been given for its fast mode of action. However, some dermatologists are now treating these very sick patients with first-line systemic anti-tumour necrosis factor alpha preparations such as infliximab.
KEY POINTS
• Erythroderma is when almost the entire skin ( 90%) becomes red.
• It is a serious and at times life-threatening dermatological emergency.
• Management is supportive in addition to treatment of the underlying cause.
need an explanation for this answer? contact us directly to get an explanation for this answer