


History
A 26-week-old baby boy attends your clinic with his mother. He has developed a gen-eralized dry, red, itchy rash over the past seven weeks. His mother has been applying a regular emollient diligently and using a bath emollient. She reports that he is waking more and more frequently at night and appears to be troubled by his skin. She is worried about weaning him. He is currently breast-fed and his mother has an unrestricted diet. He has been offered a bottle of formula milk, but took only 60 mL before vomiting and developing a rash. He also developed a rash when his father kissed him, immediately after eating an egg mayonnaise sandwich. He is the first baby of his parents; his mother had asthma in childhood and his father is allergic to shellfish. There are no pets at home. His father is a smoker. The baby was born at term by normal vaginal delivery and is vaccinated to date.
Examination
His height has reached a plateau over the past eight weeks and now rests on the 9th centile for his age. He is alert and happy, although he rubs his legs vigorously when undressed. He has generally dry skin, with widespread low-grade erythema and raised, poorly defined patches of active eczema; there are widespread excoriations (Fig. 1.1) and no clinical evidence of impetiginization. He has low-grade generalized shotty lymphad-enopathy. The rest of his examination is normal.

Questions
• What is this eruption?
• What associated condition does he pre-sent with?
• What dietary recommendations will you make for the baby (and mother)?
 Medicine
Medicine
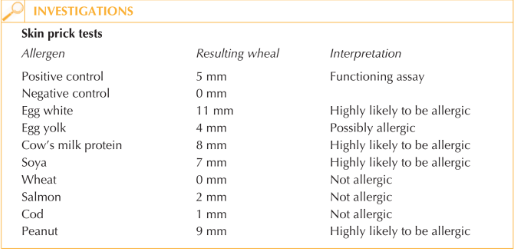
This eruption is eczema. The history his mother gives makes an associated food allergy probable – likely to egg and cow’s milk protein (CMP). This, in combination with a posi-tive family history of food allergy and asthma, means we can classify his skin condition as atopic eczema. His mother is correct to be anxious about weaning him. It would be appropriate for this baby to be investigated for associated food allergy. Food allergy is more likely in babies presenting with eczema from a young age, and it is pos-sible that food allergy may be contributing to the activity of his eczema and vice versa. The first line investigation should be skin prick test (SPT) to the common weaning food protein allergens (CMP, egg, soya, wheat, and fish). Peanut is commonly added to thisinitial panel.
The history suggests that this baby is likely to be allergic to egg and CMP, and this has been confirmed by SPT. It would be worth restricting his mother’s intake of these proteins if she intends to continue breast-feeding as this may improve eczema control.
If his mother wishes to stop breast-feeding, the most appropriate alternative at his age would be an amino acid formula. The incidence of coexisting CMP and soya allergy is high and the positive SPT would suggest this baby is currently allergic to both. CMP and egg are nutritionally important and ensuring a balanced diet while restricting both can be challenging; specialist dietetic advice is important. Low-grade exposure to allergenic proteins through maternal milk might be contributing to skin signs and his static growthparameters.
Regular use of topical emollients and avoidance of detergents are essential for main-taining the skin barrier function of infants with eczema. It is unlikely, however, that emollients and dietary restriction alone will suffice in the management of his eczema.
His parents should be introduced to the practical aspects of topical therapy and a ‘step-up, step-down’ approach to the management of flares. They should be taught to identify flares early and initiate effective therapy quickly.
The association of early-onset eczema and egg allergy is associated with a three-fold increased risk of asthma in later childhood. This is an important opportunity to discuss the potential contribution paternal smoking would have on increasing that risk. Reassuringly, both egg and CMP allergy are frequently outgrown, although peanut allergy is more likely to persist.
KEY POINTS
• Atopic eczema frequently presents within the first year of life and early onset is associated with risk of associated food allergy.
• Eczema before the age of 1 year and egg allergy are associated with an increased risk of developing asthma.
• Appropriate allergy testing and dietary advice will help prevent unsupervised dietary manipulation by well-meaning but misguided parents and may help improve eczema control.
need an explanation for this answer? contact us directly to get an explanation for this answer