


A BOY WITH DELAYED PUBERTY
History
Paul, who is 14 years and 6 months old, comes to see his GP for the first time in years. He is worried about his short stature and lack of pubertal development. He feels he is losing out in team sports and wants to become a physical education teacher. The GP records show that his father is on the 9th centile and his mother is between the 9th and 25th centiles. There are no other symptoms or past history of note.
Examination
Paul is a fit, healthy, slim boy. General and systems examination are normal. His penis is about 5 cm long and the skin of the scrotum is lax and slightly pigmented. Both testes are descended but are quite small. There is no pubic or axillary hair. Both height and weight are on the 2nd centile. The GP puts together a growth chart from the available data (see Fig. 19.1).
Figure 19.1 Paul’s growth chart. (Chart reproduced with kind permission of the Child Growth Foundation.)
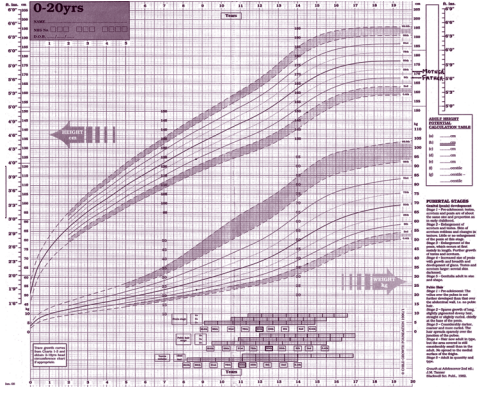
Figure 19.1 Paul’s growth chart. (Chart reproduced with kind permission of the Child Growth Foundation.)
Questions
• What is the most likely diagnosis?
• What should the GP do next?
• Is there any treatment available?
 Medicine
Medicine
The most likely diagnosis is constitutional delay of growth and puberty (CDGP) in a boy from a relatively short family. Boys enter puberty any time from 9 to 14 years old and it takes 4–5 years to complete. Puberty follows a recognized pattern with initial enlargement of the testes that produce testosterone and gradual development of secondary sexual characteristics according to Tanner stages 1 (prepubertal) to 5 (adult) – a scoring system for genital and hair development. Testicular volume can be estimated using a Prader orchidometer, 4 mL defining the onset of puberty and 15–25 mL being an adult male. This boy is only at stage 2 for genital development and stage 1 for pubic hair. Testosterone is a poor growth promoter in low concentrations (unlike oestrogen in females) so the growth spurt of puberty peaks relatively late (stage 4). Girls enter puberty between 8 and 13 years of age, hit their peak height velocity at around stage 3 and stop growing sooner than boys. Hence women are shorter than men. Constitutional delay of growth and puberty is common in boys and can be a source of misery and behaviour problems. Boys who also come from a short family may feel very different from their peer group at a time when conforming is important. This boy’s growth failure is apparent due to the current cross-sectional charts falsely depicting all boys having their growth spurt simultaneously. Unlike longitudinal charts, they take no account of the age range of normal puberty. Boys with CDGP continue to grow at their prepubertal rate, crossing the centiles downwards with later acceleration and catch-up. A family history is common. CDGP is rare in girls and a pathological cause for significant pubertal delay should be sought. The fact that the boy has summoned the courage to seek advice means he is worried. Understandably, many give an air of bravado to cover their embarrassment. Ask about bullying and teasing. Many are satisfied with reassurance that all will be well in the end, but this boy is unlikely to start his growth spurt for 12–18 months. Unless the boy is clearly reassured, the GP should refer him to the endocrine clinic. Treatment is usually available with a short course of low-dose, 4-weekly testosterone injections to give a ‘boost’ to pubertal development and thereby a growth spurt. This will have no adverse effect on final height. Usually the diagnosis is clear and no investigations are necessary except for a bone age which usually shows delay. The latter is reassuring to the family in that it demonstrates that there is additional growth potential and that the child is likely to continue to grow after his peers have stopped. If there is any uncertainty about the diagnosis, the endocrine clinic will institute further investigations.
KEY POINTS
• Conforming to their peer group is very important for adolescents.
• Constitutional delay of growth and puberty is a rarer diagnosis in girls and a pathological cause should be sought.
need an explanation for this answer? contact us directly to get an explanation for this answer