


A SHORT GIRL
History
Tanya is a 4-year-old girl brought to the GP by her mother, who is worried about her daughter’s growth. She has noticed that her shoe size has not changed for almost 12 months and she is still in clothes for a 2- to 3-year-old. She was born at 38 weeks by normal delivery and weighed 2.1 kg (9th centile). Her mother tried breast-feeding but she was never easy to feed, even with a bottle. She is generally healthy, apart from recurrent ear infections that have needed grommet insertion. She wears glasses for longsightedness. Her development is normal, although nursery staff have reported that she seems to have poor concentration.
Examination
She is generally healthy and certainly well nourished. The GP notices wide-spaced nipples and a low hairline but can find no other obvious abnormalities. She creates a growth chart from her own and the mother’s records (Fig. 16.1).
Figure 16.1 Tanya’s growth chart showing available height and weight data. (Chart reproduced with kind permission of the Child Growth Foundation.
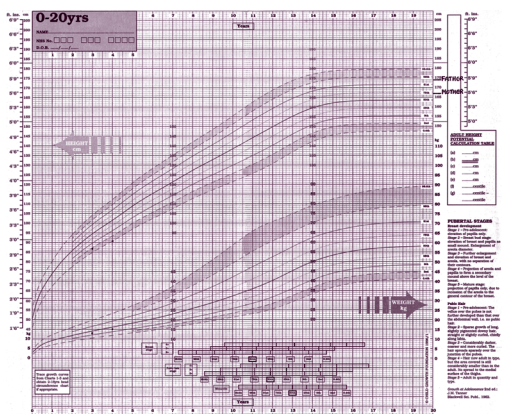
Figure 16.1 Tanya’s growth chart showing available height and weight data. (Chart reproduced with kind permission of the Child Growth Foundation.
Questions
• How did the GP plot the parents’ heights?
• What are the clinical signs that suggest a pathological cause for short stature?
• What is the most likely diagnosis?
 Medicine
Medicine
Plotting the parents’ centiles establishes whether a child falls into the expected height range for their family. Both parents should be measured, but realistically this is often difficult. To plot the father’s centile on a girls’ chart, 14 cm is subtracted from his height, and on a boys’ chart the same measurement is added to the mother’s height. Alternatively, their centile is taken from the relevant chart. The ‘target centile range’ can also be calculated. This is the midpoint of the two plotted parental centiles 8.5 cm for a girl and 10 cm for a boy. With normal parents and healthy children, final heights will be normally distributed within these 95 per cent confidence limits. Growth is unique to childhood and an excellent tool for confirming health as well as spotting disease. Children who are healthy grow and gain weight normally and follow centiles. The challenge in assessing a short child is to pick out those with a pathological cause from the majority without. Usually there is no one defining feature and pieces of the clinical jigsaw are put together from the history, examination, growth pattern and any investigations. A short child following the 0.4th to 2nd centiles from a short family is less worrying than one who is crossing the centiles downwards due to abnormally slow growth. The causes are numerous – chronic disease (coeliac disease, uncontrolled asthma), drug effects (steroids), endocrine disorders (hypothyroidism, growth hormone deficiency) and emotional abuse. Thorough clinical assessment is crucial.
Clinical signs suggesting a pathological cause for short stature
• Extreme short stature – on or below 0.4th centile.
• Short for family size – outside target range for parents
• Short and relatively overweight – suggests an endocrinopathy
• Short and very underweight – suggests poor nutrition malabsorption
• Growth failure – crossing the centiles downwards
• Dysmorphic features
• Skeletal disproportion – charts available for ratio between sitting height and leg length. Significant disproportion suggests a skeletal dysplasia, e.g. achondroplasia
• Signs of systemic disease, e.g. clubbing
This girl is extremely short, crossing the centiles, short for family and has some subtle dysmorphic features. Pathology is probable. She is also relatively overweight for height, suggesting an endocrinopathy. The GP should refer her to a growth clinic. The most likely diagnosis is Turner syndrome (TS) caused by the complete or partial absence of one of the X chromosomes. The incidence is 1 in 3000 live female births. Short stature is universal and there are specific Turner growth charts. The dysmorphic features vary in frequency (e.g. only 50 per cent have neck webbing) and are often subtle. This girl has wide-spaced nipples and a low hairline. She also has some of the other associations – low birth weight, difficult to feed in infancy, middle ear disease, visual problems and poor concentration. None of these are specific, but put together they make TS likely. Investigations must include chromosome analysis.
KEY POINTS
• Most children seen with short stature do not have a pathological cause.
• Dysmorphic features in Turner syndrome may be subtle and there should be a low threshold for chromosome analysis in all short girls.
need an explanation for this answer? contact us directly to get an explanation for this answer