


AN INCIDENTAL MURMUR
History
Lola is a 3-year-old girl referred to outpatients by her GP, who heard a murmur when she presented to him with a fever and a cough. Looking through her notes, the murmur was not heard at her 6-week check and she has only been seen twice since, with minor infections. He brought her back a week later to listen again, the murmur was still present and he has referred her on. She is otherwise entirely healthy with no significant past medical or family history.
Examination
Lola looks generally healthy and her height and weight are on the 75th centiles. She is not clinically anaemic, jaundiced or cyanosed. Her pulse is 88/min and her blood pressure 90/50 mmHg. She has normal femoral pulses. Examination of the praecordium shows no thrills but there is a heave at the lower left sternal border. The apex beat is in the fifth intercostal space in the mid-clavicular line. Both heart sounds are present but the pulmonary component of the second sound is quiet. There is a click immediately after the first heart sound and an ejection systolic murmur which is heard loudest in the pulmonary area. This radiates into both lung fields and is heard in the back between the scapulae. Examination of the respiratory and abdominal systems is normal with no hepatomegaly.
INVESTIGATIONS
Lola’s electrocardiogram is shown in Figure 12.1.
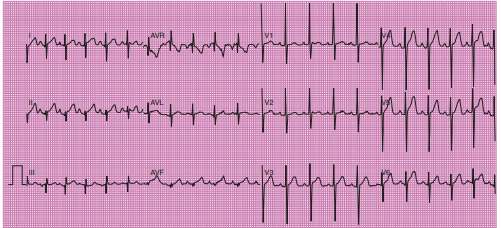
Figure 12.1 Lola’s electrocardiogram.
Questions
• Why did the GP bring her back to listen again?
• What features suggest that a murmur is innocent?
• What is the most likely diagnosis?
• What does the ECG show?
• What should happen next?
 Medicine
Medicine
Up to 40 per cent of children will have a murmur heard at some time during childhood, particularly if examined at a time of high cardiac output – e.g. fever, anaemia or anxiety. These ‘innocent’ murmurs have certain reassuring features and the heart is structurally normal. It is good practice to re-examine asymptomatic healthy children 1–2 weeks later when they are well. If the murmur persists, they should be referred. That it was not heard at the 6-week check is irrelevant – murmurs in children are often difficult to hear. A murmur can be diagnosed as innocent on the basis of the certain clinical findings (see box)
Clinical findings in innocent murmurs
• Asymptomatic
• No thrills or heaves
• Normal heart sounds, normally split with no added clicks
• Quiet and soft
• Systolic (isolated diastolic murmurs are never innocent)
• Short, ejection (pansystolic murmurs are pathological)
• Single site with no radiation to neck, lung fields or back
• Varies with posture (decreases or disappears when patient sits up, loudest when they’re lying)
Further investigations are rarely indicated. Nevertheless parents are understandably anxious and must be reassured that an innocent murmur is simply a ‘noise’. It may never disappear but this does not matter because the heart is normal. All other murmurs should be investigated. However, a normal ECG and chest X-ray do not exclude pathology. An echocardiogram is the definitive test. The findings are characteristic of moderate pulmonary valve stenosis (PS). This is common, accounting for 7–10 per cent of all congenital heart defects. Unless the stenosis is severe, children are otherwise healthy and asymptomatic. An ‘opening’ click may be heard at the beginning of systole. With increasing severity, the clinical features change to reflect the progressive narrowing and the resulting right ventricular hypertrophy (RVH). The pulmonary component of the second heart sound diminishes and a lower left sternal heave develops. In severe PS there may be evidence of right-sided heart failure with hepatomegaly. The ECG will show the same progression. This child's ECG shows right axis deviation and evidence of RVH (an ‘R' in V1 > 20 millimetres, an ‘S' in V6 > 5 millimetres and upright T waves across all the right precordial leads).
She needs an echocardiogram to:
• confirm the clinical diagnosis
• assess severity to guide further investigation and treatment
• exclude any associated cardiac lesions, e.g. ventricular septal defect.
Doppler echocardiography measures velocity across the valve – the higher this is, the greater the need for intervention. Catheter balloon valvuloplasty is the treatment of choice in the majority and the outcomes are good. Milder degrees of PS need regular re-evaluation to monitor any progression. Antibiotic prophylaxis to prevent infective endocarditis is no longer recommended in this condition.
KEY POINTS
• Cardiac murmurs are heard at some time in up to 40 per cent of children.
• The majority of murmurs in children are innocent.
• A normal ECG and chest X-ray do not exclude a pathological murmur.
• An echocardiogram is the definitive investigation.
need an explanation for this answer? contact us directly to get an explanation for this answer